CASE 77

1. What could cause this pattern of late gadolinium enhancement? (Choose all that apply.)
A. Pericarditis
B. Myocarditis
C. Amyloidosis
D. Sarcoidosis
E. Infarction
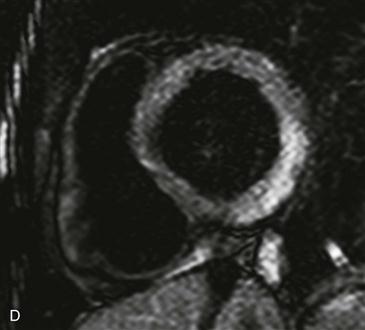
2. What sequence is shown in Fig. D?
B. Steady-state free precession (SSFP)
3. What is the likely diagnosis given the patient history and imaging findings?
A. Pericarditis
B. Myocarditis
C. Sarcoidosis
4. What is the gold standard for diagnosing this entity?
B. MRI
C. Troponin
D. Biopsy
ANSWERS
References
Deux JF, Maatouk M, Lim P, et al. Acute myocarditis: diagnostic value of contrast-enhanced cine steady-state free precession MRI sequences. AJR Am J Roentgenol. 2011;197(5):1081–1087.
Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000;343(19):1388–1398.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 91–92, 292–294.
Comment
Imaging
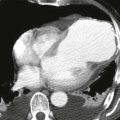
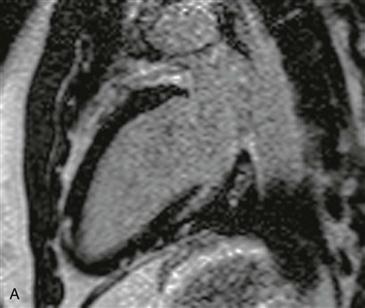
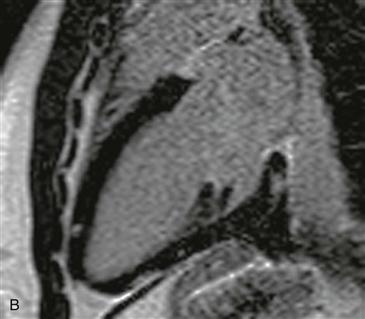
Inversion recovery late gadolinium enhancement images show nodular enhancement sparing the endocardium in the left ventricle, which does not correspond to a vascular distribution (Figs. A–C). T2-weighted black blood imaging shows hyperintensity along the inferior and lateral ventricular walls corresponding to the site of late gadolinium enhancement (Fig. D).
Epidemiology and Symptoms
Myocarditis is an inflammatory disease of the myocardium, which in the United States most commonly follows a viral infection. It occurs as secondary to the virus itself or as an immune-mediated response to viral antigens. Other causes of myocarditis include bacterial and parasitic infections and certain cardiotoxic drugs (i.e., anthracyclines and trastuzumab). Chagas disease is the most common cause worldwide. Most patients are relatively asymptomatic, and the diagnosis is discovered in postmortem studies. Symptomatic patients present with chest pain, heart failure, arrhythmia, or sudden cardiac death. Myocarditis is an important cause of sudden death in young patients (<40 years old), accounting for 12% to 20% of cases.
Diagnosis with MRI
MRI is a useful imaging modality in patients with suspected myocarditis. The acute and subacute phases of disease are characterized by T2 hyperintensity within involved myocardium (Fig. D). There is usually no late gadolinium enhancement unless irreversible damage has occurred (Figs. A–C). Early abnormalities predominate in the epicardial left ventricular free wall, the interventricular septum, and occasionally the right ventricle. Late gadolinium enhancement signifies irreversible damage or fibrosis. Specific patterns of enhancement include patchy, diffuse, nodular, or transmural, which does not follow a typical vascular territory.