Procedure 76 Percutaneous Pinning of Distal Radius Fractures
 See Video 57: Percutaneous Pinning of Distal Radius Fractures
See Video 57: Percutaneous Pinning of Distal Radius Fractures



Examination/Imaging










Exposures
 The radial-sided pins are placed first. A 2-cm incision is made over the radial styloid (Fig. 76-2).
The radial-sided pins are placed first. A 2-cm incision is made over the radial styloid (Fig. 76-2).
 The soft tissue flaps are elevated, and the skin is retracted. Branches of the superficial nerve are identified and carefully protected (Fig. 76-3).
The soft tissue flaps are elevated, and the skin is retracted. Branches of the superficial nerve are identified and carefully protected (Fig. 76-3).
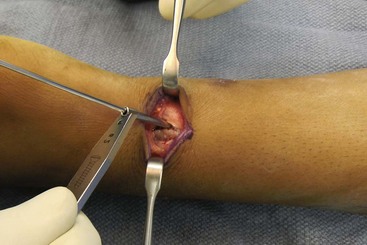
 The tip of the radial styloid is identified, and the periosteum is elevated. The tendons of the first and second dorsal compartments are reflected off the radius enough to safely insert two pins. The tendons are left within the compartments and are elevated subperiosteally (Fig. 76-4).
The tip of the radial styloid is identified, and the periosteum is elevated. The tendons of the first and second dorsal compartments are reflected off the radius enough to safely insert two pins. The tendons are left within the compartments and are elevated subperiosteally (Fig. 76-4).



Procedure
Step 1
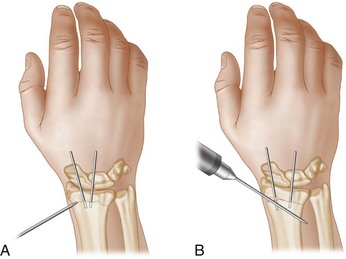
 The radial styloid pins are inserted using a soft tissue protector. The first pin is placed into the distal fragment only. The pins are typically 0.062-inch Kirschner wires (Fig. 76-5).
The radial styloid pins are inserted using a soft tissue protector. The first pin is placed into the distal fragment only. The pins are typically 0.062-inch Kirschner wires (Fig. 76-5).
 The wrist and distal fragment are flexed over a towel bump to reduce the displacement or angulation of the fracture. With the fracture reduced, a dorsoulnar pin is placed percutaneously. This pin is placed at the dorsoulnar corner of the distal radius (Fig. 76-6).
The wrist and distal fragment are flexed over a towel bump to reduce the displacement or angulation of the fracture. With the fracture reduced, a dorsoulnar pin is placed percutaneously. This pin is placed at the dorsoulnar corner of the distal radius (Fig. 76-6).

Step 1 Pearls
The radial styloid can be easily fragmented, and multiple passes of the K-wires should be avoided.
If there is difficulty in reducing the fracture, a blunt elevator can be placed percutaneously. This can be inserted into the fracture site dorsally and used to lever the fracture into a reduced position.
Step 2
 With the wrist flexed and the fracture reduced, the pins in the distal fragment are driven across the fracture and into and through the cortex of the proximal shaft.
With the wrist flexed and the fracture reduced, the pins in the distal fragment are driven across the fracture and into and through the cortex of the proximal shaft.
 An additional pin is placed from the radial styloid and across the fracture.
An additional pin is placed from the radial styloid and across the fracture.
 Anteroposterior and lateral images should show good alignment of the fracture with restoration of volar tilt and ulnar inclination (Fig. 76-7A and B).
Anteroposterior and lateral images should show good alignment of the fracture with restoration of volar tilt and ulnar inclination (Fig. 76-7A and B).

Step 2 Pearls
If the bone is very osteopenic and is not held by the pins well, then an intrafocal Kapandji technique can be used. The pins are placed through the fracture site on the dorsoradial and dorsoulnar side of the distal fragment and thereby buttress the fragment in place.
The fracture is first elevated with an osteotome and levered volarly to restore the volar tilt (Fig. 76-8A). A K-wire is then placed at the same level but driven into the intact volar cortex to hold the buttressed fragment. Additional wires can be driven along the dorsal fracture, and the radial edge of the fracture can also be elevated to restore the radial inclination (Fig. 76-8B).
At times, a combination of intrafocal pinning and pinning through the fracture fragments can be used (Fig. 76-9A and B).

Step 3




Step 4
 The technique is also useful for displaced pediatric fractures. Appropriate fractures are transphyseal or metaphyseal. Radiographs demonstrate a displaced, nonreducible physeal fracture in a 15-year-old boy (Fig. 76-10A and B).
The technique is also useful for displaced pediatric fractures. Appropriate fractures are transphyseal or metaphyseal. Radiographs demonstrate a displaced, nonreducible physeal fracture in a 15-year-old boy (Fig. 76-10A and B).
 Closed reduction and percutaneous pinning are usually easily achieved with general anesthesia and muscular paralysis (Fig. 76-11A and B).
Closed reduction and percutaneous pinning are usually easily achieved with general anesthesia and muscular paralysis (Fig. 76-11A and B).
 Pins are removed after 4 to 5 weeks in the clinic. Final radiographs should show a healed fracture with good alignment of the articular surface (Fig. 76-12A and B).
Pins are removed after 4 to 5 weeks in the clinic. Final radiographs should show a healed fracture with good alignment of the articular surface (Fig. 76-12A and B).



Postoperative Care and Expected Outcomes
 Patients are seen after 2 weeks for a dressing change and suture removal.
Patients are seen after 2 weeks for a dressing change and suture removal.
 Finger and elbow range of motion (ROM) is allowed after 2 weeks.
Finger and elbow range of motion (ROM) is allowed after 2 weeks.
 In adults, the K-wires are removed in the office 5 to 6 weeks after surgery.
In adults, the K-wires are removed in the office 5 to 6 weeks after surgery.
 Final radiographs at healing should show good alignment of the articular surface. After the pins are removed, there may be some settling of the distal fragment (Fig. 76-13A and B).
Final radiographs at healing should show good alignment of the articular surface. After the pins are removed, there may be some settling of the distal fragment (Fig. 76-13A and B).

Harley BJ, Schargenberger A, Beaupre LA, et al. Augmented external fixation versus percutaneous pinning and casting for unstable fractures of the distal radius—a prospective randomized trial. J Hand Surg [Am]. 2004;29:815-824.
Lenoble E, Dumontier C, Goutallier D, Apoil A. Fracture of the distal radius: a prospective comparison between trans-styloid and Kapandji fixations. J Bone Joint Surg [Br]. 1995;77:562-567.
Naidu SH, Capo JT, Moulton M, et al. Percutaneous pinning of distal radius fractures: a biomechanical study. J Hand Surg [Am]. 1997;22:252-257.
Trumble TE, Wagner W, Hanel DP, et al. Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg [Am]. 1998;23:381-394.


