Procedure 75 Scaphotrapeziotrapezoid Arthrodesis and Lunate Excision with Replacement by Palmaris Longus Tendon
Indications




Examination/Imaging
Clinical Examination





Imaging
Plain Radiographs
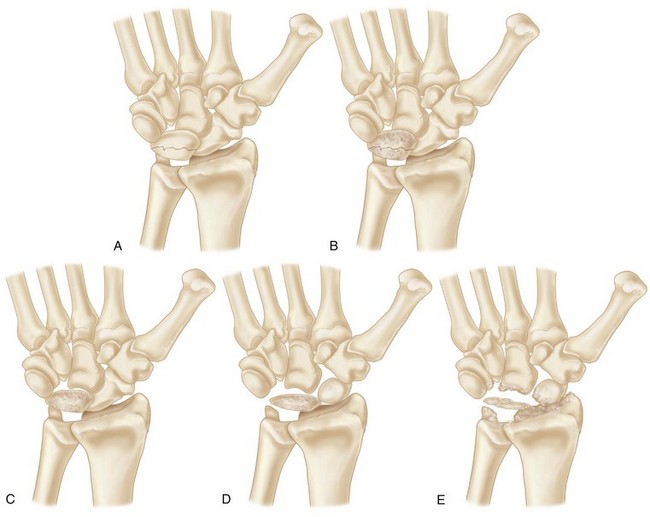
 Staging: Lichtman modification of Stahl staging
Staging: Lichtman modification of Stahl staging
 Posteroanterior (PA) and lateral radiographs with the wrist in neutral rotation and neutral flexion-extension (Fig. 75-2).
Posteroanterior (PA) and lateral radiographs with the wrist in neutral rotation and neutral flexion-extension (Fig. 75-2).

 Lunate sclerosis, carpal instability patterns, and fragmentation are seen.
Lunate sclerosis, carpal instability patterns, and fragmentation are seen.

 Evaluation of relationship among scaphoid, trapezium, and trapezoid.
Evaluation of relationship among scaphoid, trapezium, and trapezoid.

Computed Tomography
 Computed tomography (CT) is needed to evaluate precisely the bony architecture of the lunate and the remainder of the carpus to determine which procedure is indicated and to determine whether arthritic changes of the midcarpal and radiocarpal joints are present.
Computed tomography (CT) is needed to evaluate precisely the bony architecture of the lunate and the remainder of the carpus to determine which procedure is indicated and to determine whether arthritic changes of the midcarpal and radiocarpal joints are present.
 A CT scan is useful for evaluation of fragmentation or fracture patterns and associated collapse.
A CT scan is useful for evaluation of fragmentation or fracture patterns and associated collapse.




Controversies

Treatment Options
Radial shortening osteotomy and capitate shortening may also unload the lunate.
Instead of STT arthrodesis, some surgeons prefer to perform scaphocapitate (SC) arthrodesis.
Revascularization with a vascularized bone graft has been advocated in early stages, and successes have been reported in late stages as well.
Core decompression of the lunate has also been described.
Salvage procedures for painful wrists that have not responded to the STT arthrodesis include total wrist arthrodesis, partial or total wrist arthroplasty, or proximal row carpectomy.



Exposures

Procedure
 Superficial branches of the radial nerve are retracted during the procedure.
Superficial branches of the radial nerve are retracted during the procedure.
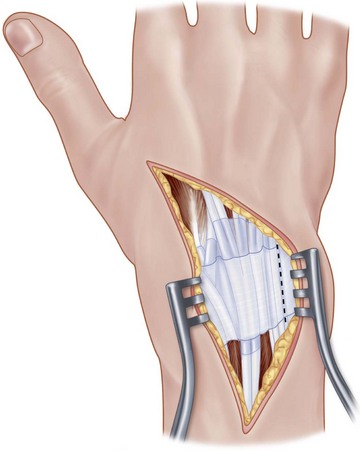
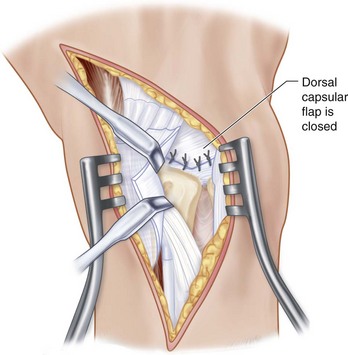
 Through the proximal half of the incision, the extensor retinaculum is exposed. The capsular flap is incised between the third and fourth dorsal compartments to expose the lunate (Fig. 75-5).
Through the proximal half of the incision, the extensor retinaculum is exposed. The capsular flap is incised between the third and fourth dorsal compartments to expose the lunate (Fig. 75-5).
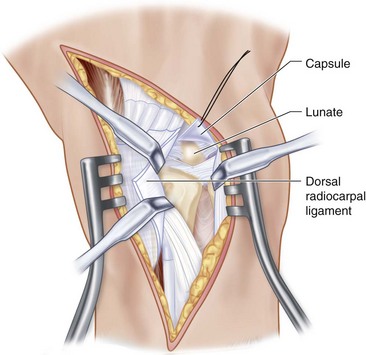
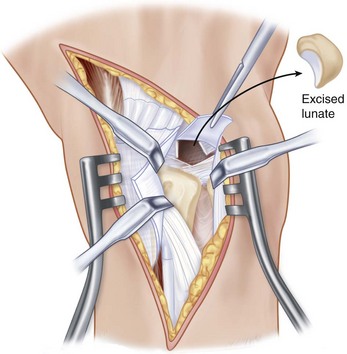
 The lunate is removed piecemeal or entirely in one piece, with great care to avoid injury to the palmar wrist ligaments (Fig. 75-6).
The lunate is removed piecemeal or entirely in one piece, with great care to avoid injury to the palmar wrist ligaments (Fig. 75-6).
 An ipsilateral palmaris longus tendon is removed with a tendon stripper.
An ipsilateral palmaris longus tendon is removed with a tendon stripper.


Instrumentation/Implantation
Various types of small osteotomes and chisels are useful to remove the cortex of scaphoid, trapezium, and trapezoid. A low-powered surgical bur is also convenient to expose cancellous bones between the scaphoid, trapezium, and trapezoid.
A hand-held drill is necessary to insert K-wires between the scaphoid, trapezium, and trapezoid.
Step 1 Pitfalls
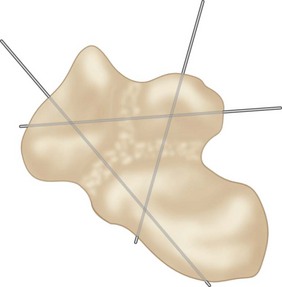
The lunate is ideally removed as one bone, although this is not easy. Therefore, we prefer to remove the lunate piecemeal.
The palmar wrist capsule and ligaments are protected during removal of the lunate.
If the palmaris longus tendon is absent, the plantaris tendon or a half slip of the extensor carpi radialis longus tendon is harvested.
Step 2
 Through the distal half of the incision, the wrist and thumb extensors are exposed.
Through the distal half of the incision, the wrist and thumb extensors are exposed.
 Wrist and thumb extensors are retracted.
Wrist and thumb extensors are retracted.
 The articular surfaces between the scaphoid, trapezium, and trapezoid are exposed.
The articular surfaces between the scaphoid, trapezium, and trapezoid are exposed.
 The articular cartilage and subchondral bone of the three joints are removed to expose the cancellous bone (Fig. 75-8).
The articular cartilage and subchondral bone of the three joints are removed to expose the cancellous bone (Fig. 75-8).
 Cancellous bone from the iliac crest is grafted into the joint spaces to prevent shortening of the carpus (Fig. 75-9).
Cancellous bone from the iliac crest is grafted into the joint spaces to prevent shortening of the carpus (Fig. 75-9).

Step 3
 The proximal pole of the scaphoid is depressed until it is under the dorsal surface of the lunate fossa on the radius to reduce the flexed posture of the scaphoid. This distal pole is pulled dorsally, if necessary, and K-wires are then driven percutaneously through the scaphoid into the capitate to maintain reduction (see Fig. 75-9).
The proximal pole of the scaphoid is depressed until it is under the dorsal surface of the lunate fossa on the radius to reduce the flexed posture of the scaphoid. This distal pole is pulled dorsally, if necessary, and K-wires are then driven percutaneously through the scaphoid into the capitate to maintain reduction (see Fig. 75-9).
 The position of the scaphoid is confirmed by intraoperative imaging (Fig. 75-10).
The position of the scaphoid is confirmed by intraoperative imaging (Fig. 75-10).
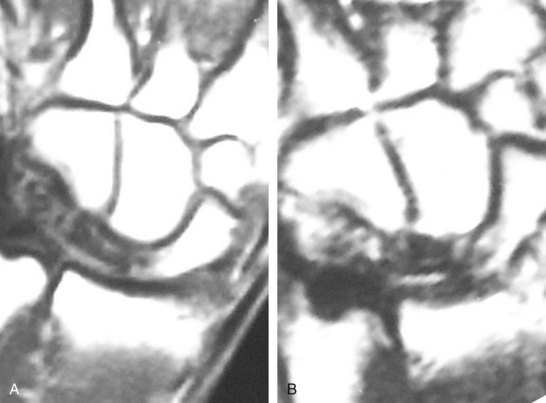
 Figure 75-10A shows a preoperative radiograph of Kienböck disease classified by stage IIIB.
Figure 75-10A shows a preoperative radiograph of Kienböck disease classified by stage IIIB.
 Figure 75-10B shows a radiograph of the excision of the lunate.
Figure 75-10B shows a radiograph of the excision of the lunate.
 Figure 75-10C shows a radiograph of an STT arthrodesis after the removal of the lunate.
Figure 75-10C shows a radiograph of an STT arthrodesis after the removal of the lunate.
 Figure 75-10D shows a radiograph 3 years after excision of the lunate and STT arthrodesis.
Figure 75-10D shows a radiograph 3 years after excision of the lunate and STT arthrodesis.




Postoperative Care and Expected Outcomes





Minami A, Kato H, Suenaga N, et al. Scaphotrapezio-trapezoid fusion: long-term follow-up study. J Orthop Sci.. 2003;8:319-322.
Minami A, Kimura T, Suzuki K. Long-term results of Kienböck’s disease treated by triscaphe arthrodesis and excisional arthroplasty with a coiled palmaris longus tendon. J Hand Surg [Am]. 1994;19:219-228.
Watson HK, Ryu J, DiBella A. An approach to Kienböck’s disease: Triscaphe arthrodesis. J Hand Surg [Am]. 1985;10:17-87.


