CASE 75

1. What should be included in the differential diagnosis? (Choose all that apply.)
A. Myocarditis
B. Infarction
C. Ischemia
E. Sarcoidosis
2. What is the likely diagnosis if this patient had long-standing bilateral hilar lymphadenopathy?
A. Myocarditis
B. Infarction
D. Sarcoidosis
3. Which organ or system is most commonly affected by sarcoidosis?
B. Heart
C. Liver
4. What type of cardiomyopathy is most commonly associated with sarcoidosis?
A. Dilated
B. Restrictive
C. Hypertrophic
ANSWERS
References
Smedema JP, Snoep G, van Kroonenburgh MP, et al. Evaluation of the accuracy of gadolinium-enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. J Am Coll Cardiol. 2005;45(10):1683–1690.
Youssef G, Beanlands RS, Birnie DH, Nery PB. Cardiac sarcoidosis: applications of imaging in diagnosis and directing treatment. Heart. 2011;97(24):2078–2087.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 89, 92.
Comment
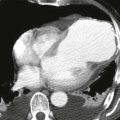
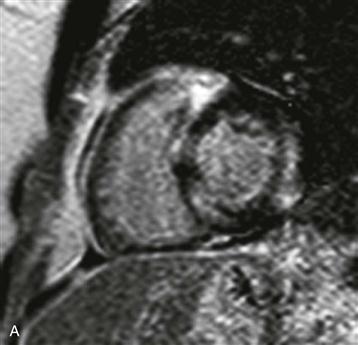
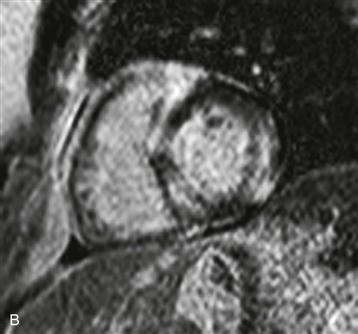
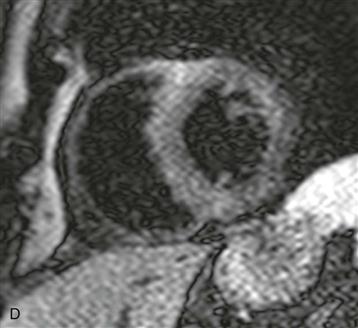
Imaging
Short-axis and four-chamber images show patchy late gadolinium enhancement that does not follow a typical vascular distribution and spares the subendocardial layer (Figs. A–C). T2-weighted black blood short-axis image shows no hyperintensity to indicate active inflammation (Fig. D). This patient had pulmonary sarcoidosis and was given a presumptive diagnosis of cardiac sarcoidosis based on the MRI findings.
Epidemiology
Myocardial involvement by sarcoidosis is uncommon, clinically affecting approximately 5% of all patients with the disease. Autopsy series show cardiac involvement in 27% of asymptomatic patients. The cardiovascular system is the third most commonly affected organ system. When the heart is involved, patients may be asymptomatic but are at greater risk for acute heart failure, arrhythmia, and sudden cardiac death. Sarcoidosis most commonly affects the myocardium; specifically, there is often sparing of the subendocardium with involvement of the basal septum, left ventricular free wall, and right ventricular free wall.