Procedure 72 Dorsal Capsulodesis for Scapholunate Instability Using Suture Anchors
 See Video 53: Dorsal Capsulodesis for Scapholunate Ligament Injury
See Video 53: Dorsal Capsulodesis for Scapholunate Ligament Injury
Indications
 Static or dynamic dorsal intercalated segmental instability (DISI) deformity is found without a wide scapholunate (SL) gap.
Static or dynamic dorsal intercalated segmental instability (DISI) deformity is found without a wide scapholunate (SL) gap.
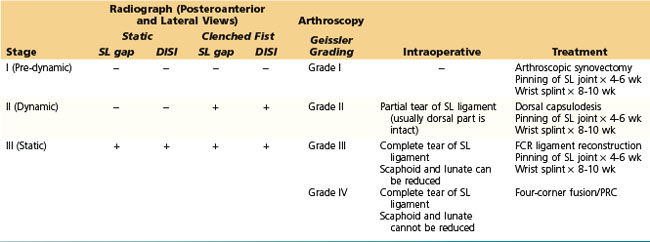
 We determine the treatment for SL instability based on clinical presentation, radiographic appearance, and arthroscopic and intraoperative findings. Our current algorithm for selection of appropriate procedure for SL instability is indicated in Table 72-1.
We determine the treatment for SL instability based on clinical presentation, radiographic appearance, and arthroscopic and intraoperative findings. Our current algorithm for selection of appropriate procedure for SL instability is indicated in Table 72-1.
Examination/Imaging
Clinical Examination
 Patients complain of radial-sided wrist pain especially with loading activities, weakness of grip, and swelling, along with discomfort at extremes of wrist extension and radial deviation.
Patients complain of radial-sided wrist pain especially with loading activities, weakness of grip, and swelling, along with discomfort at extremes of wrist extension and radial deviation.



Imaging
 Stress views, including the clenched-fist view, posteroanterior maximal radial deviation, and posteroanterior maximal ulnar deviation, are useful in the diagnosis of dynamic SL instability.
Stress views, including the clenched-fist view, posteroanterior maximal radial deviation, and posteroanterior maximal ulnar deviation, are useful in the diagnosis of dynamic SL instability.
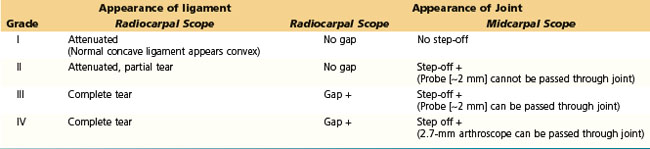
 Arthroscopic examination has become the standard method of evaluation of interosseous ligamentous injuries. The arthroscopic classification of ligament injuries proposed by Geissler (Table 72-2) is useful in determining treatment options.
Arthroscopic examination has become the standard method of evaluation of interosseous ligamentous injuries. The arthroscopic classification of ligament injuries proposed by Geissler (Table 72-2) is useful in determining treatment options.
Surgical Anatomy
 The SL ligament is a C-shaped structure that connects the dorsal, proximal, and volar surfaces of the scaphoid and lunate. Partial SL ligament tears most often involve only the proximal and volar components of the SL interosseous ligament complex. The dorsal ligament is much stronger than its volar counterpart and may resist substantial traumatic torques without yielding.
The SL ligament is a C-shaped structure that connects the dorsal, proximal, and volar surfaces of the scaphoid and lunate. Partial SL ligament tears most often involve only the proximal and volar components of the SL interosseous ligament complex. The dorsal ligament is much stronger than its volar counterpart and may resist substantial traumatic torques without yielding.


Exposures
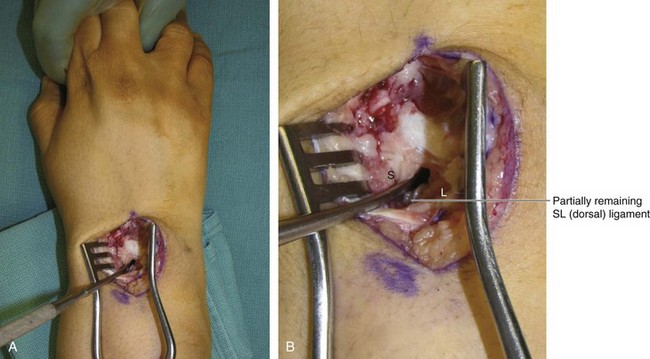
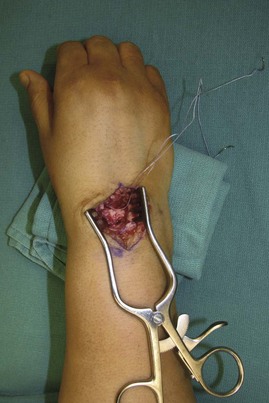
 A 6-cm dorsal longitudinal incision centered over the radiocarpal joint in line with the long finger metacarpal is made (Fig. 72-1). Sharp dissection is carried down to the extensor retinaculum. Skin and subcutaneous tissue flaps are raised on both sides. The third dorsal compartment is identified and does not need to be opened along its entire length. The wrist capsule is opened longitudinally and dissection performed to elevate the second and fourth compartments, such that the second and fourth compartment tendons are maintained within the compartment (Fig. 72-2). This exposes the scaphoid and lunate.
A 6-cm dorsal longitudinal incision centered over the radiocarpal joint in line with the long finger metacarpal is made (Fig. 72-1). Sharp dissection is carried down to the extensor retinaculum. Skin and subcutaneous tissue flaps are raised on both sides. The third dorsal compartment is identified and does not need to be opened along its entire length. The wrist capsule is opened longitudinally and dissection performed to elevate the second and fourth compartments, such that the second and fourth compartment tendons are maintained within the compartment (Fig. 72-2). This exposes the scaphoid and lunate.
 Figure 72-3 shows a Freer elevator within the SL interval demonstrating a partial rupture of the SL dorsal ligament.
Figure 72-3 shows a Freer elevator within the SL interval demonstrating a partial rupture of the SL dorsal ligament.


Procedure
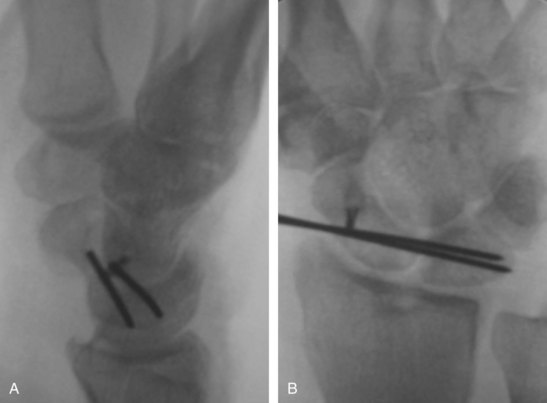
Step 1: Reduction of Scaphoid and Lunate

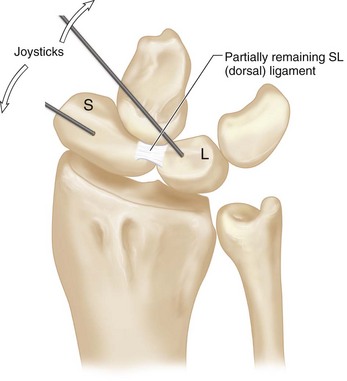
Step 2: Maintenance of SL Reduction


Step 3: Make a Drill Hole in the Scaphoid, and Insert a Bone Anchor
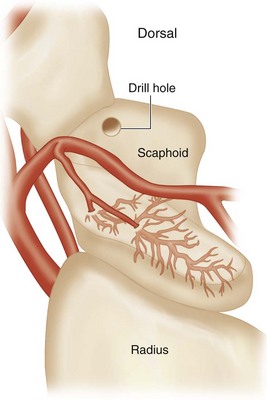
 Make a drill hole at the most distal part of the scaphoid (Fig. 72-5).
Make a drill hole at the most distal part of the scaphoid (Fig. 72-5).
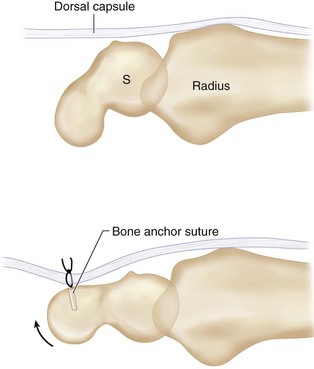
 A 1.8-mm bone anchor suture (Mitek Mini QuickAnchor or similar) is placed in the drill hole (Fig. 72-6).
A 1.8-mm bone anchor suture (Mitek Mini QuickAnchor or similar) is placed in the drill hole (Fig. 72-6).

Step 4: Secure the Dorsal Capsule to the Scaphoid







Postoperative Care and Expected Outcomes





Gajendran VK, Peterson B, Slater RRJr, Szabo RM. Long-term outcomes of dorsal intercarpal ligament capsulodesis for chronic scapholunate dissociation. J Hand Surg [Am]. 2007;32:1323-1333.
Moran SL, Cooney WP, Berger RA, Strickland J. Capsulodesis for the treatment of chronic scapholunate instability. J Hand Surg [Am]. 2005;30:16-23.
Wintman BI, Gelberman RH, Katz JN. Dynamic scapholunate instability: results of operative treatment with dorsal capsulodesis. J Hand Surg [Am]. 1995;20:971-979.

