Procedure 71 Open Reduction and Acute Repair of Perilunate Fracture-Dislocations


Examination/Imaging
Clinical Examination





Imaging
 Lunate and perilunate dislocations are occasionally missed in the emergency room and dismissed as a severe wrist sprain despite having adequate imaging. Therefore, it is essential to obtain a thorough radiographic examination and scrutinize the images to prevent missing an acute injury.
Lunate and perilunate dislocations are occasionally missed in the emergency room and dismissed as a severe wrist sprain despite having adequate imaging. Therefore, it is essential to obtain a thorough radiographic examination and scrutinize the images to prevent missing an acute injury.
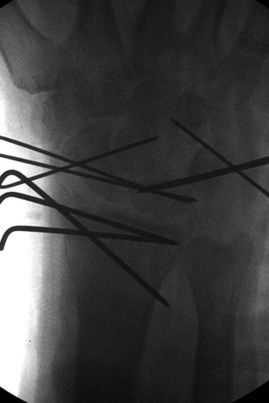
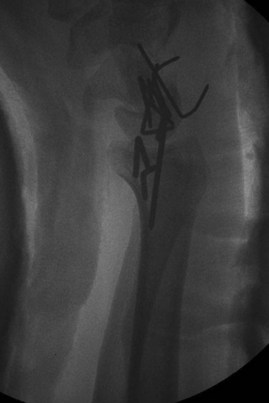
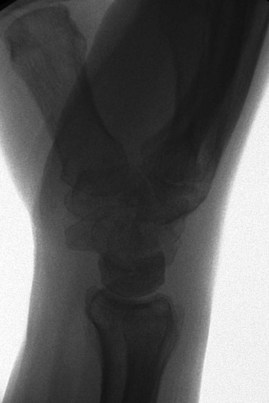
 A standard radiographic series of the wrist must be obtained to evaluate for dislocation. Assess for disruption of Gilula arc lines on the posteroanterior image. On a lateral radiograph, the radial shaft, lunate, capitate, and metacarpal shafts should be collinear (Fig. 71-1).
A standard radiographic series of the wrist must be obtained to evaluate for dislocation. Assess for disruption of Gilula arc lines on the posteroanterior image. On a lateral radiograph, the radial shaft, lunate, capitate, and metacarpal shafts should be collinear (Fig. 71-1).
 Radiographs should also be inspected to rule out associated radial styloid, scaphoid, capitate, or triquetral fractures (Fig. 71-2).
Radiographs should also be inspected to rule out associated radial styloid, scaphoid, capitate, or triquetral fractures (Fig. 71-2).
 Computed tomography can help better define any questionable fractures of the carpal bones.
Computed tomography can help better define any questionable fractures of the carpal bones.



Surgical Anatomy
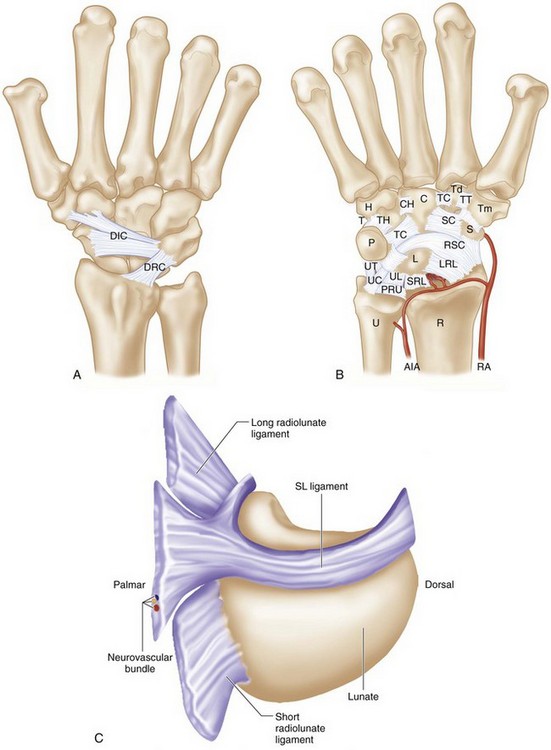
 The dorsal radiocarpal and intercarpal ligaments are frequently ruptured in these severe injuries (Fig 71-3A).
The dorsal radiocarpal and intercarpal ligaments are frequently ruptured in these severe injuries (Fig 71-3A).
 The strong volar ligaments have a characteristic transverse rent that is repaired through the volar approach (Fig. 71-3B).
The strong volar ligaments have a characteristic transverse rent that is repaired through the volar approach (Fig. 71-3B).
 The lunate dislocates through the space of Poirier, a relatively weak region of the volar capsule just below the arc of the radioscaphocapitate and ulnocapitate ligaments (see Fig. 71-3B).
The lunate dislocates through the space of Poirier, a relatively weak region of the volar capsule just below the arc of the radioscaphocapitate and ulnocapitate ligaments (see Fig. 71-3B).
 The dorsal portion of the scapholunate ligament is the thickest and strongest portion of the C-shaped ligament and should be repaired if adequate ligament tissue is present (Fig. 71-3C).
The dorsal portion of the scapholunate ligament is the thickest and strongest portion of the C-shaped ligament and should be repaired if adequate ligament tissue is present (Fig. 71-3C).

Positioning



Exposures
 A 7- to 8-cm longitudinal dorsal incision centered over the wrist is made, with exposure of the carpus through the third dorsal compartment (extensor pollicis longus [EPL] sheath).
A 7- to 8-cm longitudinal dorsal incision centered over the wrist is made, with exposure of the carpus through the third dorsal compartment (extensor pollicis longus [EPL] sheath).
 An extended carpal tunnel release incision is also made at the wrist. This extends from the Kaplan cardinal line distally to 3 to 4 cm proximal to the distal wrist flexion crease (Fig. 71-4).
An extended carpal tunnel release incision is also made at the wrist. This extends from the Kaplan cardinal line distally to 3 to 4 cm proximal to the distal wrist flexion crease (Fig. 71-4).

Procedure
Step 1: Volar Approach
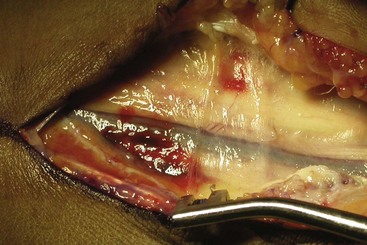
 After the extended carpal tunnel incision, dissection is carried down through the transverse carpal ligament and distal antebrachial fascia to completely decompress the median nerve (Fig. 71-5).
After the extended carpal tunnel incision, dissection is carried down through the transverse carpal ligament and distal antebrachial fascia to completely decompress the median nerve (Fig. 71-5).
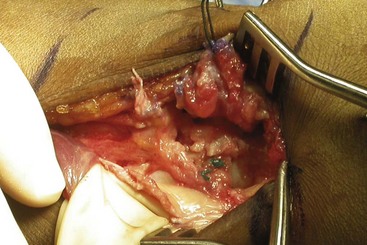
 The nerve and all flexor tendons are retracted to expose the floor of the carpal tunnel, the transverse ligamentous rent, and lunate within the carpal tunnel if it had not been previously reduced (Fig. 71-6).
The nerve and all flexor tendons are retracted to expose the floor of the carpal tunnel, the transverse ligamentous rent, and lunate within the carpal tunnel if it had not been previously reduced (Fig. 71-6).
 The lunate can be manually reduced with dorsal pressure and some longitudinal traction.
The lunate can be manually reduced with dorsal pressure and some longitudinal traction.
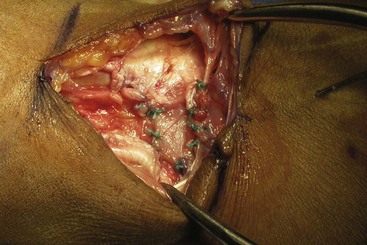
 The transverse ligamentous rent is repaired using multiple 3-0 braided nonabsorbable sutures (Fig. 71-7).
The transverse ligamentous rent is repaired using multiple 3-0 braided nonabsorbable sutures (Fig. 71-7).


Step 2: Dorsal Approach






Step 3


Step 4


Step 5






Postoperative Care and Expected Outcomes




Hildebrand KA, Ross DC, Patterson SD, et al. Dorsal perilunate dislocations and fracture-dislocations: questionnaire, clinical, and radiographic evaluation. J Hand Surg [Am]. 2000;25:1069-1079.
Trumble T, Verheyden J. Treatment of isolated perilunate and lunate dislocations with combined dorsal and volar approach and intraosseous cerclage wire. J Hand Surg [Am]. 2004;29:412-417.


