[level-membership-for-anesthesiology-category]
CHAPTER 71 Lung Isolation Techniques
1 What are the indications for lung isolation?
There are five areas for which lung isolation may be required:







2 How can lung isolation be achieved while maintaining one-lung ventilation?
3 How do you choose the appropriate size double-lumen endotracheal tube?
There are right and left DLTs to account for the anatomic differences between the right and left main stem bronchi. Most commonly left-sided tubes are used. The optimal tube size for a particular patient is the largest tube that will pass atraumatically through the glottis, advance down the trachea, and fit in the bronchus with a small air leak detectable when the cuff is deflated. Using the largest possible tube is associated with the least airway resistance and ensures that a bronchial seal is obtained with small cuff volumes. A DLT that is too small requires a large endobronchial cuff volume, which may result in cuff herniation across the carina. Many anesthesiologists select 41-Fr and 39-Fr DLTs for tall and short men, respectively, and 39-Fr and 35- to 37-Fr DLTs for tall and short women, respectively. There is considerable variation in left main stem bronchi diameters and a relatively weak predictive value of gender and height. Other alternatives to predict the size of the optimal DLT are to measure the patient’s trachea and left or right main stem bronchus diameters from preoperative radiologic studies such as chest x-ray films and computed tomography scans (Table 71-1).
TABLE 71-1 Conversion Measurements of Tracheal Width Based on Chest X-Ray and Bronchial Diameter Measurements*
| Measured Tracheal Width (mm) at Clavicles on CXR | Measured Bronchial Diameter (mm) | Left-Sided DLT (Fr) |
|---|---|---|
| ≥18 | ≥12 | 41 |
| ≥16 | 12 | 39 |
| ≥15 | 11 | 37 |
| ≥14 | 10 | 35 |
| ≥12.5 | <10 | 32 |
| ≥11 | NA | 28 |
CXR, Chest x-ray; DLT, double-lumen endotracheal tube.
* Bronchial diameter measurements based on computed tomography scan of the chest and the predicted left-sided double lumen endotracheal tube size.
Data from Brodsky JB, Macario A, Mark JBD: Tracheal diameter predicts double-lumen tube size: a method for selecting left double-lumen tubes, Anesth Analg 82:861–864, 1996; and Hannallah M, et al: Evaluation of an approach to choosing a left double-lumen tube based on chest computed tomography scan measurement of left mainstem bronchial diameter, J Cardiothorac Vasc Anesth 11:168–171, 1997.
4 How is the right main stem bronchus different from the left and how does this affect right-sided double-lumen endotracheal tube design?
 The wider right bronchus diverges away from the trachea at a 25-degree angle, whereas the left bronchus diverges at a 45-degree angle.
The wider right bronchus diverges away from the trachea at a 25-degree angle, whereas the left bronchus diverges at a 45-degree angle.

 Therefore right-sided DLTs must have a slit in the bronchial cuff for ventilating the right upper lobe. It is more difficult to correctly position a right-sided DLT because of anatomic variations between individuals in the distance between the right upper lobe orifice and the carina, often resulting in difficulties ventilating the right upper lobe (Figure 71-1).
Therefore right-sided DLTs must have a slit in the bronchial cuff for ventilating the right upper lobe. It is more difficult to correctly position a right-sided DLT because of anatomic variations between individuals in the distance between the right upper lobe orifice and the carina, often resulting in difficulties ventilating the right upper lobe (Figure 71-1).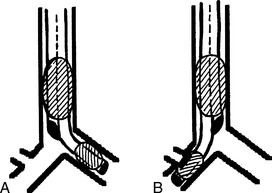
6 What complications may be caused by double-lumen endotracheal tubes?
 Malposition: Most often occurs when a patient is turned from the supine to the lateral position. Usually there is cephalad movement of the DLT by 1 cm. Malposition can be avoided by maintaining the head in a neutral position with folded blankets to avoid flexion and extension. After repositioning, the FOB should be used to confirm that the DLT is still in good position.
Malposition: Most often occurs when a patient is turned from the supine to the lateral position. Usually there is cephalad movement of the DLT by 1 cm. Malposition can be avoided by maintaining the head in a neutral position with folded blankets to avoid flexion and extension. After repositioning, the FOB should be used to confirm that the DLT is still in good position.

12 What complications can occur with the Univent tube?
There are two serious complications with improper use of the Univent tube:
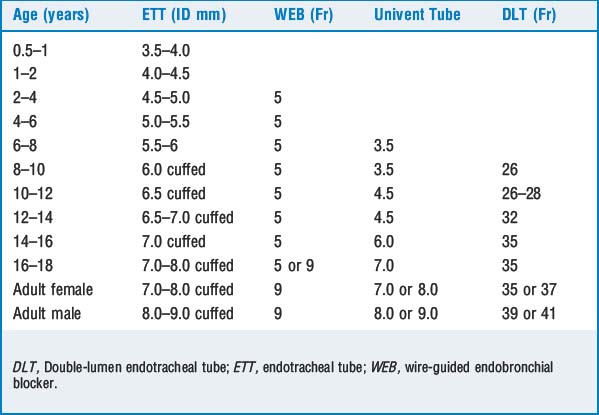
16 What tubes or bronchial blockers would you select for single-lung ventilation in children and adults?
KEY POINTS: Lung Isolation 










1. Brodsky J.B., Macario A., Mark J.B.D. Tracheal diameter predicts double-lumen tube size: a method for selecting left double-lumen tubes. Anesth Analg. 1996;82:861-864.
2. Campos J.H., Hallam E.A., Van Natta T., et al. Devices for lung isolation used by anesthesiologists with limited thoracic experience: comparison of double-lumen endotracheal tube, Univent torque control blocker, and Arndt wire-guided endobronchial blocker. Anesthesiology. 2006;104:261-266.
3. Campos J.H. Which device should be considered the best for lung isolation: double-lumen endotracheal tube versus bronchial blockers. Curr Opin Anaesthesiol. 2007;20:27-31.
4. Hammer G.B. Single-lung ventilation in infants and children. Pediatr Anesth. 2004;14:98-102.
5. Hannallah M., et al. Evaluation of an approach to choosing a left double-lumen tube based on chest computed tomography scan measurement of left mainstem bronchial diameter. J Cardiothorac Vasc Anesth. 1997;11:168-171.
6. Knoll H., Ziegeler S., Schreiber J.U., et al. Airway injuries after one-lung ventilation: a comparison between double-lumen tube and endobronchial blocker: a randomized, prospective, controlled trial. Anesthesiology. 2006;105:471-477.
7. Ovassapian A. Fiber-optic endoscopy and the difficult airway, ed 2. Philadelphia: Lippincott-Raven, 1996.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 71 Lung Isolation Techniques
1 What are the indications for lung isolation?
There are five areas for which lung isolation may be required:
2 How can lung isolation be achieved while maintaining one-lung ventilation?
3 How do you choose the appropriate size double-lumen endotracheal tube?
There are right and left DLTs to account for the anatomic differences between the right and left main stem bronchi. Most commonly left-sided tubes are used. The optimal tube size for a particular patient is the largest tube that will pass atraumatically through the glottis, advance down the trachea, and fit in the bronchus with a small air leak detectable when the cuff is deflated. Using the largest possible tube is associated with the least airway resistance and ensures that a bronchial seal is obtained with small cuff volumes. A DLT that is too small requires a large endobronchial cuff volume, which may result in cuff herniation across the carina. Many anesthesiologists select 41-Fr and 39-Fr DLTs for tall and short men, respectively, and 39-Fr and 35- to 37-Fr DLTs for tall and short women, respectively. There is considerable variation in left main stem bronchi diameters and a relatively weak predictive value of gender and height. Other alternatives to predict the size of the optimal DLT are to measure the patient’s trachea and left or right main stem bronchus diameters from preoperative radiologic studies such as chest x-ray films and computed tomography scans (Table 71-1).
TABLE 71-1 Conversion Measurements of Tracheal Width Based on Chest X-Ray and Bronchial Diameter Measurements*
| Measured Tracheal Width (mm) at Clavicles on CXR | Measured Bronchial Diameter (mm) | Left-Sided DLT (Fr) |
|---|---|---|
| ≥18 | ≥12 | 41 |
| ≥16 | 12 | 39 |
| ≥15 | 11 | 37 |
| ≥14 | 10 | 35 |
| ≥12.5 | <10 | 32 |
| ≥11 | NA | 28 |
CXR, Chest x-ray; DLT, double-lumen endotracheal tube.
* Bronchial diameter measurements based on computed tomography scan of the chest and the predicted left-sided double lumen endotracheal tube size.
Data from Brodsky JB, Macario A, Mark JBD: Tracheal diameter predicts double-lumen tube size: a method for selecting left double-lumen tubes, Anesth Analg 82:861–864, 1996; and Hannallah M, et al: Evaluation of an approach to choosing a left double-lumen tube based on chest computed tomography scan measurement of left mainstem bronchial diameter, J Cardiothorac Vasc Anesth 11:168–171, 1997.
4 How is the right main stem bronchus different from the left and how does this affect right-sided double-lumen endotracheal tube design?
The wider right bronchus diverges away from the trachea at a 25-degree angle, whereas the left bronchus diverges at a 45-degree angle. Therefore right-sided DLTs must have a slit in the bronchial cuff for ventilating the right upper lobe. It is more difficult to correctly position a right-sided DLT because of anatomic variations between individuals in the distance between the right upper lobe orifice and the carina, often resulting in difficulties ventilating the right upper lobe (Figure 71-1).