Procedure 70 Medial Femoral Condyle Vascularized Bone Flap for Scaphoid Nonunion
 See Video 52: Free Medial Femoral Condyle Vascularized Bone Transfer for Scaphoid Nonunion
See Video 52: Free Medial Femoral Condyle Vascularized Bone Transfer for Scaphoid Nonunion
Indications




Examination/Imaging






Surgical Anatomy
Recipient Site: Vascular Anatomy of Scaphoid
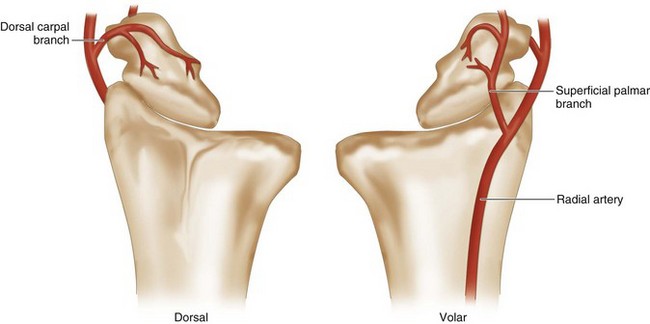
 The major blood supply to the scaphoid is through the radial artery, which enters through the dorsal ridge and supplies 70% to 80% of the intraosseous vascularity to the entire proximal pole. This vessel and its branches enter distally and dorsally in retrograde fashion to the scaphoid. The dorsal vessels travel proximally along the dorsal scaphoid ridge, and the majority of vessels enter the scaphoid waist and continue as intraosseous vessels. The scaphoid proximal pole is uniquely susceptible to avascular necrosis following fracture owing to high dependence on a single dominant retrograde traveling intraosseous vessel (Fig. 70-1).
The major blood supply to the scaphoid is through the radial artery, which enters through the dorsal ridge and supplies 70% to 80% of the intraosseous vascularity to the entire proximal pole. This vessel and its branches enter distally and dorsally in retrograde fashion to the scaphoid. The dorsal vessels travel proximally along the dorsal scaphoid ridge, and the majority of vessels enter the scaphoid waist and continue as intraosseous vessels. The scaphoid proximal pole is uniquely susceptible to avascular necrosis following fracture owing to high dependence on a single dominant retrograde traveling intraosseous vessel (Fig. 70-1).

Donor Site: Medial Femoral Condyle
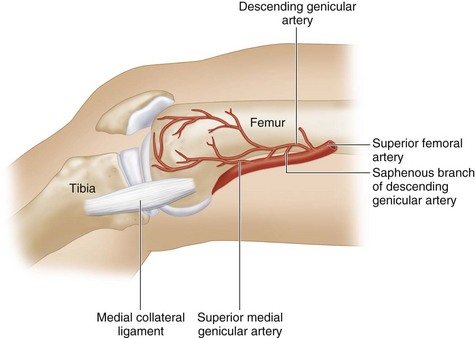
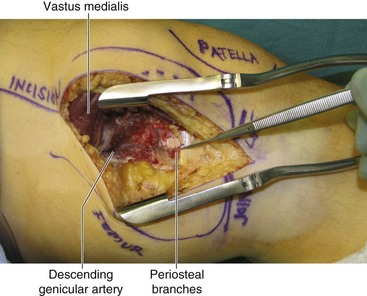
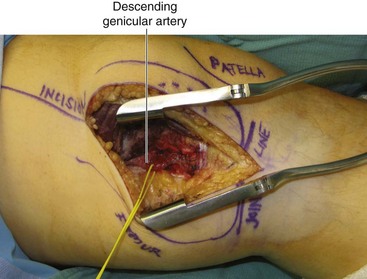
 The superficial femoral artery gives off the descending genicular artery branch just proximal to the adductor hiatus. The descending genicular artery travels distally and gives off a saphenous branch proximally and musculare branches distally. The superior medial genicular artery arises from the superficial femoral artery more distally.
The superficial femoral artery gives off the descending genicular artery branch just proximal to the adductor hiatus. The descending genicular artery travels distally and gives off a saphenous branch proximally and musculare branches distally. The superior medial genicular artery arises from the superficial femoral artery more distally.

 The saphenous branch of the descending genicular artery supplies the medial femoral condyle skin flap (Fig. 70-2).
The saphenous branch of the descending genicular artery supplies the medial femoral condyle skin flap (Fig. 70-2).

Exposures
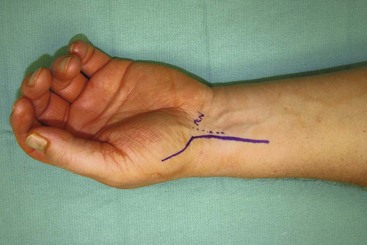
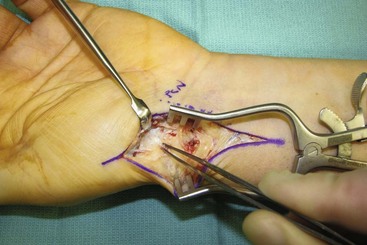
 The scaphoid and radial artery are exposed by a palmar incision. This curvilinear incision extends proximally from the radial aspect of the thenar eminence parallel and radial to the flexor carpi radialis (Fig. 70-3).
The scaphoid and radial artery are exposed by a palmar incision. This curvilinear incision extends proximally from the radial aspect of the thenar eminence parallel and radial to the flexor carpi radialis (Fig. 70-3).
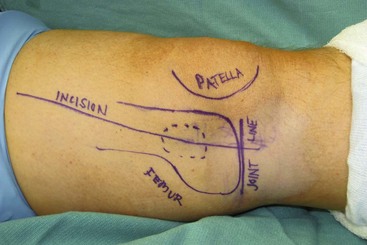
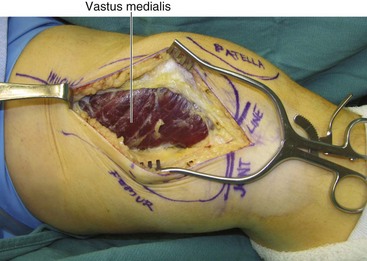
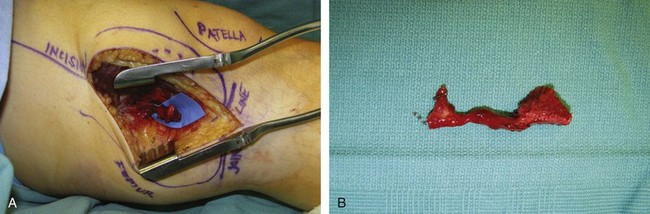
 The medial femoral condyle of the ipsilateral medial knee and its nutrient vessels are exposed using a longitudinal lower medial thigh incision (Fig. 70-4).
The medial femoral condyle of the ipsilateral medial knee and its nutrient vessels are exposed using a longitudinal lower medial thigh incision (Fig. 70-4).
Procedure
Team 1: Donor Site (Bone Graft Harvest)
Step 1

Step 2


Step 3

Step 4

Step 5


Step 6
 The periosteum is sharply incised using a no. 15 blade, and the bone is cut with a small osteotome along the marking line (Fig. 70-8).
The periosteum is sharply incised using a no. 15 blade, and the bone is cut with a small osteotome along the marking line (Fig. 70-8).
Step 7






Team 2: Recipient Site Preparation and Microanastomosis

Step 2
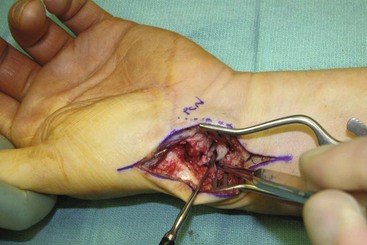
 The FCR sheath is opened, the tendon retracted ulnarly, and the floor of the FCR tunnel sharply incised longitudinally to expose the radiocarpal joint at the level of the scaphoid (Fig. 70-10).
The FCR sheath is opened, the tendon retracted ulnarly, and the floor of the FCR tunnel sharply incised longitudinally to expose the radiocarpal joint at the level of the scaphoid (Fig. 70-10).
Step 2 Pearls
The radioscaphocapitate (RSC) and long radiolunate (LRL) ligaments are identified and incised. Much of the LRL and a portion of the RSC are left intact to help stabilize the proximal pole.
Preserving this ligamentous support also helps maintain fracture reduction.
Volar capsulotomy in the scaphotrapezial joint is performed to improve the visualization of the scaphoid.
Step 3
 The scaphoid is then examined, paying attention to the articular cartilage of the radioscaphoid and midcarpal joints.
The scaphoid is then examined, paying attention to the articular cartilage of the radioscaphoid and midcarpal joints.
 A Freer elevator is used to define the location of the nonunion and the borders of the scaphoid.
A Freer elevator is used to define the location of the nonunion and the borders of the scaphoid.
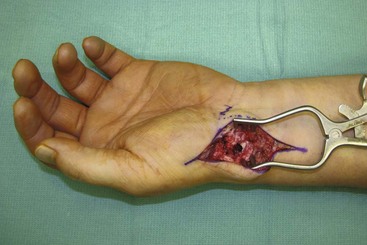
 Fibrous and/or necrotic tissues at the proximal and distal poles are examined carefully. A small curet or rongeur is used for débridement and removal of intervening fibrotic tissue (Fig. 70-11).
Fibrous and/or necrotic tissues at the proximal and distal poles are examined carefully. A small curet or rongeur is used for débridement and removal of intervening fibrotic tissue (Fig. 70-11).
Step 4




Step 5



Step 7
 The bone graft harvested from the medial femoral condyle is further shaped to fit the defect.
The bone graft harvested from the medial femoral condyle is further shaped to fit the defect.
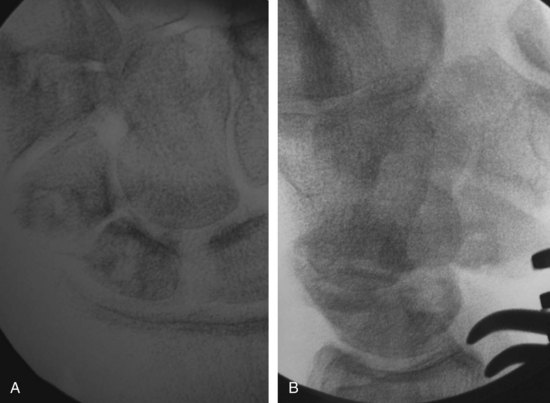
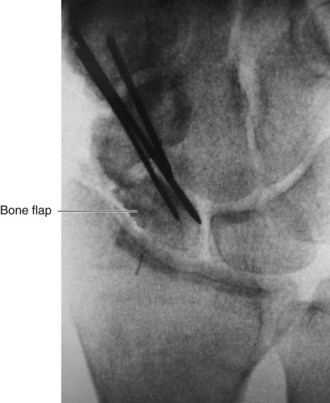
 The flap is inserted into the defect, and Kirschner wires (or headless cannulated screws) are passed through the scaphoid and bone flap for fixation under fluoroscopic imaging to confirm correction of the scaphoid shortening and DISI deformity (Fig. 70-14).
The flap is inserted into the defect, and Kirschner wires (or headless cannulated screws) are passed through the scaphoid and bone flap for fixation under fluoroscopic imaging to confirm correction of the scaphoid shortening and DISI deformity (Fig. 70-14).

Step 8
 The recipient artery (descending genicular artery or superior medial genicular artery) is anastomosed to the radial artery in an end-to-side fashion using 9-0 nylon sutures under microscopic magnification.
The recipient artery (descending genicular artery or superior medial genicular artery) is anastomosed to the radial artery in an end-to-side fashion using 9-0 nylon sutures under microscopic magnification.
 The venae comitantes of the descending genicular artery or superior medial genicular artery is anastomosed to the venae comitantes of the radial artery or to the cephalic vein in an end-to-end fashion by 9-0 nylon sutures (Fig. 70-15).
The venae comitantes of the descending genicular artery or superior medial genicular artery is anastomosed to the venae comitantes of the radial artery or to the cephalic vein in an end-to-end fashion by 9-0 nylon sutures (Fig. 70-15).





Postoperative Care and Expected Outcomes



Doi K, Hattori Y. Vascularized bone graft from the supracondylar region of the femur. Microsurgery. 2009;29:379-384.
Jones DBJr, Burger H, Shin AY, et al. Treatment of scaphoid waist nonunions with an avascular proximal pole and carpal collapse: a comparison of two vascularized bone grafts. J Bone Joint Surg [Am]. 2008;90:2616-2625.


