[level-membership-for-surgery-category]
Procedure 7 Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
 See Video 4: Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
See Video 4: Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
Indications





Examination/Imaging
Clinical Examination







Surgical Anatomy
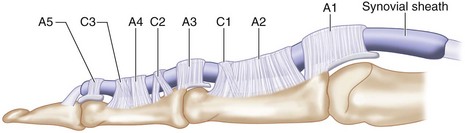
 Flexor zone 1 is distal to flexor digitorum superficialis (FDS) insertion over the middle third of the middle phalanx and contains only the FDP, C3, and A5 pulleys (Fig. 7-3).
Flexor zone 1 is distal to flexor digitorum superficialis (FDS) insertion over the middle third of the middle phalanx and contains only the FDP, C3, and A5 pulleys (Fig. 7-3).
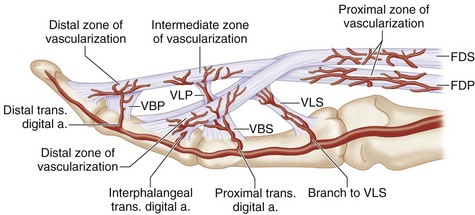
 Blood supply to the distal FDP is from the vinculum longus profundus (VLP), vinculum brevis profundus (VBP), and distal phalanx at its bony insertion (Fig. 7-4).
Blood supply to the distal FDP is from the vinculum longus profundus (VLP), vinculum brevis profundus (VBP), and distal phalanx at its bony insertion (Fig. 7-4).
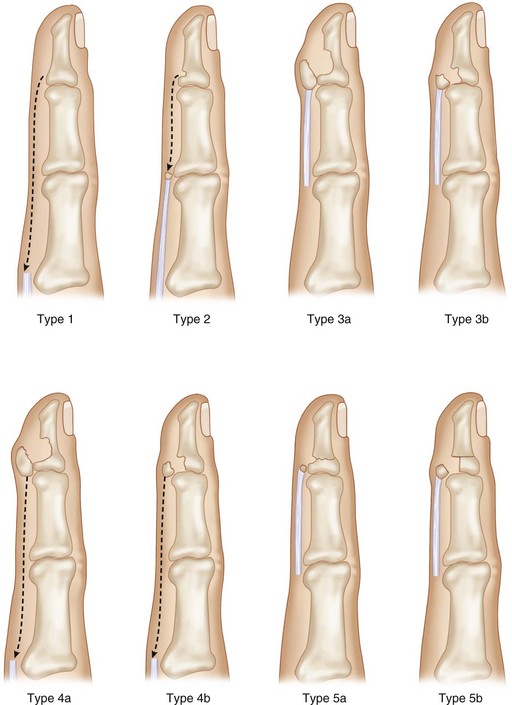
 Avulsed tendon can retract proximally in three patterns as defined by Leddy and Packer (1977). Additional types 4 and 5 have been described (Fig. 7-5).
Avulsed tendon can retract proximally in three patterns as defined by Leddy and Packer (1977). Additional types 4 and 5 have been described (Fig. 7-5).





Exposures
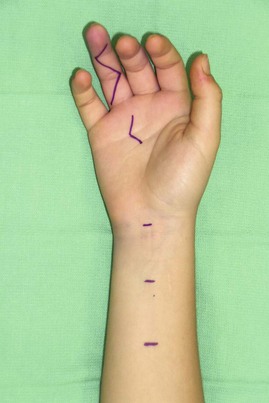
 A zigzag Bruner incision will provide the best exposure of the finger. The incision can be extended proximally as needed to retrieve the tendon or provide exposure for repair (Fig. 7-6).
A zigzag Bruner incision will provide the best exposure of the finger. The incision can be extended proximally as needed to retrieve the tendon or provide exposure for repair (Fig. 7-6).

Procedure
Step 1
 Exploration of the finger with a zigzag incision is used to identify the proximal tendon at one of several classic locations—at A4, between A2 and A4 pulleys, or at A1 (Fig. 7-7).
Exploration of the finger with a zigzag incision is used to identify the proximal tendon at one of several classic locations—at A4, between A2 and A4 pulleys, or at A1 (Fig. 7-7).
 The A2 pulley is partially opened to retrieve the proximal tendon (Fig. 7-8).
The A2 pulley is partially opened to retrieve the proximal tendon (Fig. 7-8).
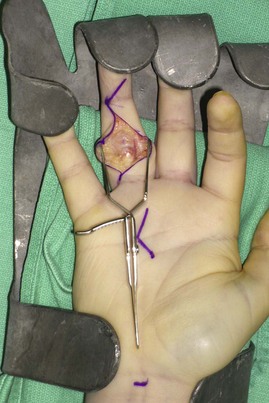
 At the distal tendon insertion, thin atrophic tendon remains that is not suitable for repair (Fig. 7-9).
At the distal tendon insertion, thin atrophic tendon remains that is not suitable for repair (Fig. 7-9).
 Excursion of the proximal tendon is tested and found to be inadequate for tension-free repair (Fig. 7-10).
Excursion of the proximal tendon is tested and found to be inadequate for tension-free repair (Fig. 7-10).

 This provides additional mobility of tendon to allow primary repair (Fig. 7-11).
This provides additional mobility of tendon to allow primary repair (Fig. 7-11).
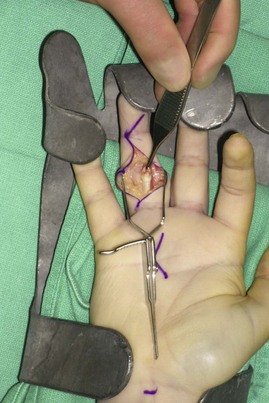
 A small feeding catheter is gently threaded through the A2 pulley into the palmar incision (Fig. 7-12). The feeding catheter is sutured to the proximal profundus tendon using a horizontal mattress suture, and the tendon is gently threaded through the pulley system into the distal incision (Fig. 7-13).
A small feeding catheter is gently threaded through the A2 pulley into the palmar incision (Fig. 7-12). The feeding catheter is sutured to the proximal profundus tendon using a horizontal mattress suture, and the tendon is gently threaded through the pulley system into the distal incision (Fig. 7-13).
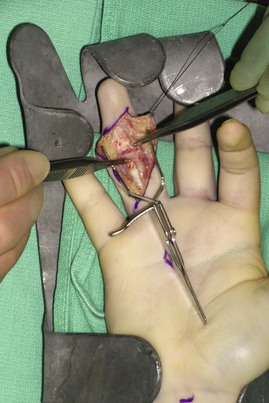
 The wrist is flexed to decrease the tension on the profundus tendon so that more of the tendon can be retrieved into the distal incision. A needle is inserted to hold the tendon in place (Fig. 7-14).
The wrist is flexed to decrease the tension on the profundus tendon so that more of the tendon can be retrieved into the distal incision. A needle is inserted to hold the tendon in place (Fig. 7-14).





Step 2
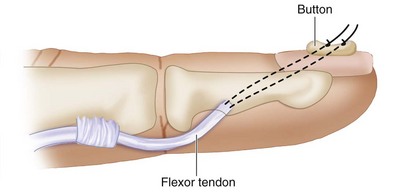
 In avulsion injuries, direct tenorrhaphy is not possible, and treatment consists of reattaching the proximal tendon to the bone via pullout suture over a button (Fig. 7-15).
In avulsion injuries, direct tenorrhaphy is not possible, and treatment consists of reattaching the proximal tendon to the bone via pullout suture over a button (Fig. 7-15).
 The distal tendon remnant and scar is resected to expose the volar base of the distal phalanx.
The distal tendon remnant and scar is resected to expose the volar base of the distal phalanx.
 The volar proximal aspect of the distal phalanx is gently débrided until cancellous bone is encountered. A bone tunnel is not necessary (Fig. 7-16).
The volar proximal aspect of the distal phalanx is gently débrided until cancellous bone is encountered. A bone tunnel is not necessary (Fig. 7-16).
 Zigzag 3-0 Prolene suture is passed through the distal end of the tendon (Fig. 7-17).
Zigzag 3-0 Prolene suture is passed through the distal end of the tendon (Fig. 7-17).


 The sutures are then secured in place with a bolster, or button, on the dorsal aspect of the finger (Fig. 7-18).
The sutures are then secured in place with a bolster, or button, on the dorsal aspect of the finger (Fig. 7-18).



Step 2 Pearls
• Prolene sutures are used because they can slide out easily upon healing of the tendon to the bone, which takes about 6 weeks.
• One must be careful when placing the Keith needles through the nail to avoid proximal penetration of the germinal matrix, which may cause nail deformity.
• When tying down the Prolene suture over the nail, the surgeon must observe the tendon sitting securely within the bone trough at the distal phalanx.
• The elevated periosteum can be sutured to the end of the tendon using 4-0 Ethibond braided suture to provide additional support.
Postoperative Care and Expected Outcomes
 The patient is placed in a dorsal blocking splint with the wrist flexed at 60 degrees and the MCP joints flexed at 90 degrees to take tension off the tendon repair site (Fig. 7-19).
The patient is placed in a dorsal blocking splint with the wrist flexed at 60 degrees and the MCP joints flexed at 90 degrees to take tension off the tendon repair site (Fig. 7-19).


 The button and the Prolene suture are removed at 8 weeks after surgery in the clinic.
The button and the Prolene suture are removed at 8 weeks after surgery in the clinic.
 Three months after the tendon repair, the patient begins strengthening exercises and continues scar massages to achieve better excursion of the flexor tendon. (Fig. 7-20 demonstrates the early postoperative result of the patient shown in Fig. 7-1.)
Three months after the tendon repair, the patient begins strengthening exercises and continues scar massages to achieve better excursion of the flexor tendon. (Fig. 7-20 demonstrates the early postoperative result of the patient shown in Fig. 7-1.)


Pitfalls
Tendon rupture is a distinct possibility if the tendon does not heal to the bone. One should immediately explore the tendon system and place a tendon graft when a rupture is encountered because the tendon sheath will collapse quickly when the sheath is empty. Early exploration is much easier because the tendon sheath is still open, and retrieval and excision of the ruptured tendon within the sheath are relatively easy. However, if the exploration is delayed, the ruptured tendon may be adherent to the pulley system and the tendon sheath may contract, which makes primary tendon grafting difficult.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 7 Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
See Video 4: Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
Indications
Examination/Imaging
Clinical Examination
Surgical Anatomy
Flexor zone 1 is distal to flexor digitorum superficialis (FDS) insertion over the middle third of the middle phalanx and contains only the FDP, C3, and A5 pulleys (Fig. 7-3).
Blood supply to the distal FDP is from the vinculum longus profundus (VLP), vinculum brevis profundus (VBP), and distal phalanx at its bony insertion (Fig. 7-4).
Avulsed tendon can retract proximally in three patterns as defined by Leddy and Packer (1977). Additional types 4 and 5 have been described (Fig. 7-5).
[/not-level-membership-for-surgery-category]
