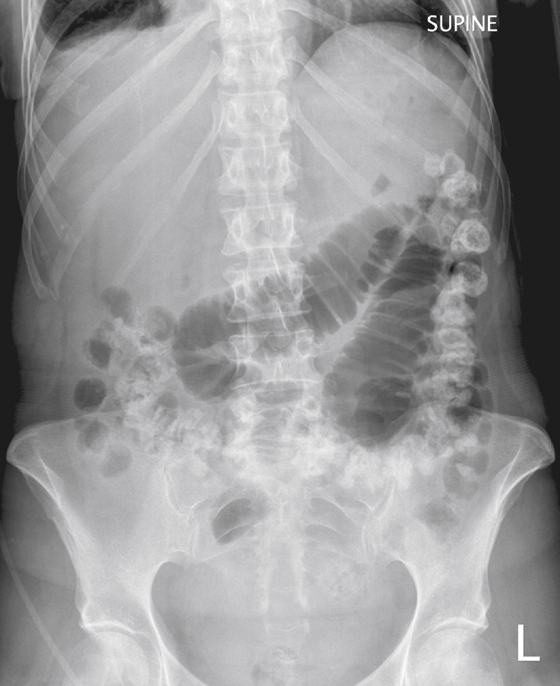

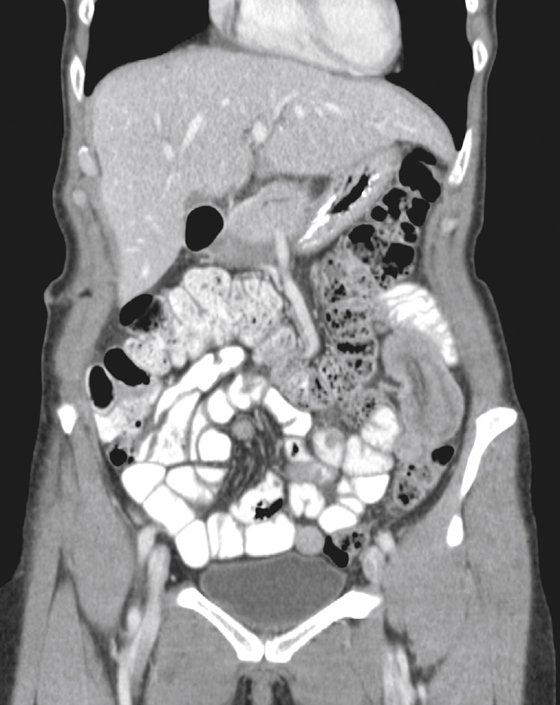

History: A 56-year-old woman underwent resection of small bowel melanoma metastases. Nine days after surgery, she developed nausea and vomiting.
1. Which of the following should be included in the differential diagnosis of the imaging findings shown for this patient? (Choose all that apply.)
2. Which of the following statements regarding small bowel tumors is true?
A. Small bowel tumors most commonly manifest with intussusception.
B. Small bowel tumors are usually benign.
C. The most common malignancy of the distal small bowel is carcinoid.
D. The most common site of small bowel lymphoma is proximal jejunum.
3. What is the most common tumor of the small bowel?
A. Gastrointestinal stromal tumor
4. Which of the following polyposis syndromes is associated with an increased risk of small bowel cancer?
ANSWERS
CASE 7
Small Bowel Intussusception
1. A and C
2. C
3. A
4. B
References
Buckley JA, Fishman EK. CT evaluation of small bowel neoplasms: spectrum of disease. Radiographics. 1998;18:379–392.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 145.
Comment
Tumors of the small bowel are not commonly encountered because they tend to occur with less frequency than esophageal, gastric, or colonic lesions; are harder to detect; and are often asymptomatic. Except for the polyposis syndromes, they are usually seen in the older population and can manifest with bleeding, intussusception, and bowel obstruction. The most common benign small bowel tumor is the gastrointestinal stromal tumor (GIST), followed by lipomas. Both lesions, as well as other benign and malignant polypoid processes, can result in a bowel intussusception. Lymphoid hyperplasia can act as the nidus for intussusception in small children.
Most cases are seen in children; only 5% to 15% of all cases of intussusception are seen in adults. Intussusceptions in adults are commonly seen when they are symptomatic and obstructed (see figure). However, most intussusceptions are probably transient, causing chronic vague abdominal symptoms that usually subside over time. Of course, when the intussusceptum (the telescoping part of the bowel) becomes locked into the intussuscipiens (the receiving part of the bowel), the symptoms are immediately evident and the situation is worsened by edema and vascular congestion, making reduction difficult (see figures). In children especially, most intussusceptions are ileocolonic and often can be reduced by slow and careful distention of the colon via a barium enema. In adults the intussusceptions tend to be ileoileum and require surgical intervention. Invariably, an adult intussusception has a polyp, benign or malignant, as the leading nidus of the intussusception (see figures).






