Procedure 69 Vascularized Bone Grafting for Scaphoid Nonunion
 See Video 51: Pedicled Vascularized Bone Transfer for Scaphoid Nonunion
See Video 51: Pedicled Vascularized Bone Transfer for Scaphoid Nonunion
Indications



Examination/Imaging
Clinical Examination



Imaging
 Wrist radiographs including scaphoid views should be obtained to evaluate the overall fracture pattern, carpal alignment, and degree of radiocarpal and midcarpal arthritis. Chronic scaphoid nonunions display a characteristic pattern of wrist arthritis and carpal instability—scaphoid nonunion advanced collapse (SNAC), as described by Watson and Ballet. The hallmark of AVN on radiographs is increased bone density, fragmentation, and collapse (Fig. 69-1).
Wrist radiographs including scaphoid views should be obtained to evaluate the overall fracture pattern, carpal alignment, and degree of radiocarpal and midcarpal arthritis. Chronic scaphoid nonunions display a characteristic pattern of wrist arthritis and carpal instability—scaphoid nonunion advanced collapse (SNAC), as described by Watson and Ballet. The hallmark of AVN on radiographs is increased bone density, fragmentation, and collapse (Fig. 69-1).

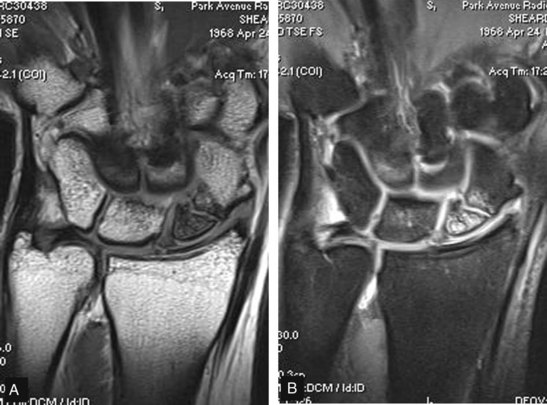
 Magnetic resonance imaging (MRI) is the only noninvasive study able to assess vascularity of the scaphoid and identify AVN (Fig. 69-2). An MRI should be obtained in every patient for whom there is a concern about the viability of the proximal pole. Contrast-enhanced imaging has a sensitivity of 66%, a specificity of 88%, and an accuracy of 83%.
Magnetic resonance imaging (MRI) is the only noninvasive study able to assess vascularity of the scaphoid and identify AVN (Fig. 69-2). An MRI should be obtained in every patient for whom there is a concern about the viability of the proximal pole. Contrast-enhanced imaging has a sensitivity of 66%, a specificity of 88%, and an accuracy of 83%.

Surgical Anatomy
 Eighty percent of the scaphoid surface is covered by articular cartilage, leaving limited space for vascular supply.
Eighty percent of the scaphoid surface is covered by articular cartilage, leaving limited space for vascular supply.
 A dorsal branch of the radial artery provides 70% to 80% of the blood supply.
A dorsal branch of the radial artery provides 70% to 80% of the blood supply.
 A second nutrient artery enters volarly and supplies only the distal pole.
A second nutrient artery enters volarly and supplies only the distal pole.
 There is no nutrient artery to the proximal pole; thus, it is susceptible to AVN when fractured.
There is no nutrient artery to the proximal pole; thus, it is susceptible to AVN when fractured.
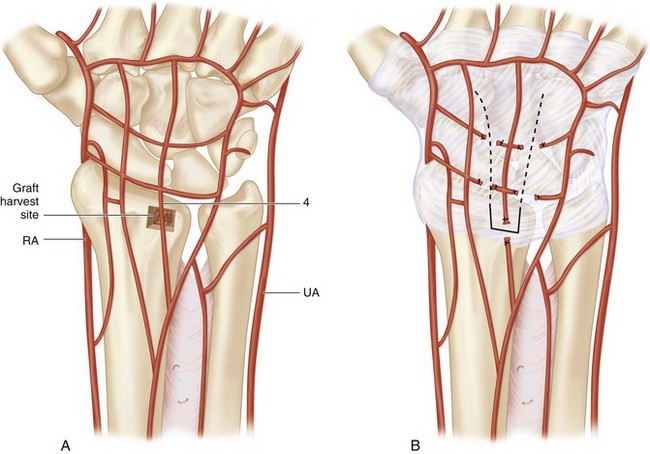
 Dorsal distal-radius vascularized bone grafts have been shown to be based on consistent vascular anatomy (Fig. 69-3A).
Dorsal distal-radius vascularized bone grafts have been shown to be based on consistent vascular anatomy (Fig. 69-3A).
 The pedicled graft described in this chapter is based on the artery of the fourth extensor compartment. The fourth extensor compartment artery is less than 1 mm in diameter and between 1 and 2 cm in length (see Fig. 69-3A and B).
The pedicled graft described in this chapter is based on the artery of the fourth extensor compartment. The fourth extensor compartment artery is less than 1 mm in diameter and between 1 and 2 cm in length (see Fig. 69-3A and B).



Exposures
 Multiple vascularized grafts have been described. One of the more popular grafts is that based on the 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) as described by Zaidemberg. We prefer to use a dorsal capsular distal-radius graft as described by Sotereanos and coworkers because it does not involve dissection of tiny vessels, is less technically demanding, and is more durable during flap rotation.
Multiple vascularized grafts have been described. One of the more popular grafts is that based on the 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) as described by Zaidemberg. We prefer to use a dorsal capsular distal-radius graft as described by Sotereanos and coworkers because it does not involve dissection of tiny vessels, is less technically demanding, and is more durable during flap rotation.
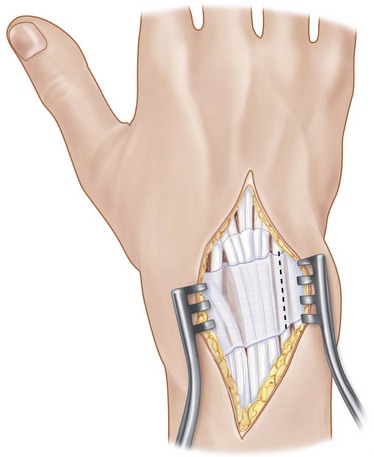
 A 4-cm dorsal incision is made centered over the radiocarpal joint, ulnar to the Lister tubercle (Fig. 69-4).
A 4-cm dorsal incision is made centered over the radiocarpal joint, ulnar to the Lister tubercle (Fig. 69-4).
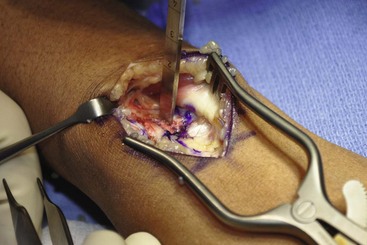
 The extensor retinaculum over the third and fourth dorsal compartments is released. The extensor pollicis longus (EPL) tendon is retracted radially and the extensor digitorum communis (EDC) tendons ulnarly, exposing the dorsal wrist capsule (Fig. 69-5).
The extensor retinaculum over the third and fourth dorsal compartments is released. The extensor pollicis longus (EPL) tendon is retracted radially and the extensor digitorum communis (EDC) tendons ulnarly, exposing the dorsal wrist capsule (Fig. 69-5).


Procedure
Step 1: Cutting the Graft



Step 2: Elevate the Graft and Pedicle
 The proximal, medial, and lateral edge osteotomies are completed with a straight osteotome (Fig. 69-7).
The proximal, medial, and lateral edge osteotomies are completed with a straight osteotome (Fig. 69-7).
 The graft is then carefully elevated with a curved osteotome, leaving 2 to 3 mm of distal radius cortex intact (Fig. 69-8).
The graft is then carefully elevated with a curved osteotome, leaving 2 to 3 mm of distal radius cortex intact (Fig. 69-8).
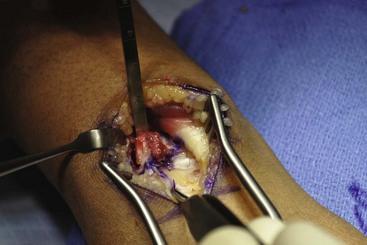
 Full-thickness dorsal capsular incisions are made, and the capsular flap is dissected away from the underlying tissues. The capsular attachment to the portion of the distal radius cortex left intact is carefully released with a scalpel. Be particularly mindful not to disturb the capsular attachment to the bone graft (Fig. 69-9).
Full-thickness dorsal capsular incisions are made, and the capsular flap is dissected away from the underlying tissues. The capsular attachment to the portion of the distal radius cortex left intact is carefully released with a scalpel. Be particularly mindful not to disturb the capsular attachment to the bone graft (Fig. 69-9).

Step 3: Scaphoid Preparation and Fixation





Step 4: Insetting the Graft
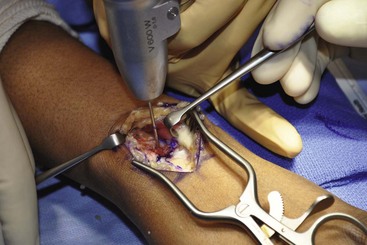
 The tourniquet is now deflated to check the viability of the graft. It may take several minutes to see punctate bleeding from the graft.
The tourniquet is now deflated to check the viability of the graft. It may take several minutes to see punctate bleeding from the graft.
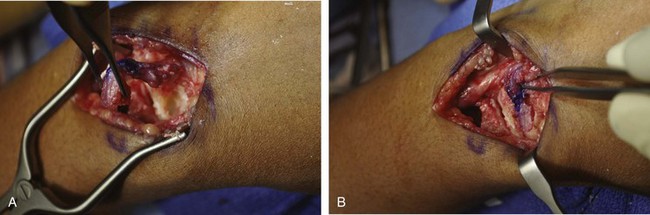
 A trough, slightly smaller than the bone block, is created on the dorsal aspect of the scaphoid with a high-speed bur. The trough should be centered over the nonunion site and deep enough to hold the bone block securely (Fig. 69-11).
A trough, slightly smaller than the bone block, is created on the dorsal aspect of the scaphoid with a high-speed bur. The trough should be centered over the nonunion site and deep enough to hold the bone block securely (Fig. 69-11).
 The bone block, attached to its capsular pedicle, is then press-fit into the trough (Fig. 69-12).
The bone block, attached to its capsular pedicle, is then press-fit into the trough (Fig. 69-12).
 Final fluoroscopic posteroanterior and lateral images after the graft was inset are shown in Figure 69-13.
Final fluoroscopic posteroanterior and lateral images after the graft was inset are shown in Figure 69-13.





Postoperative Care and Expected Outcomes


Sotereanos DG, Darlis NA, Dailiana ZH, et al. A capsular-based vascularized distal radius graft for proximal pole scaphoid pseudarthrosis. J Hand Surg [Am]. 2006;31:580-587.
Sunagawa T, Bishop AT, Muramatsu K. Role of conventional and vascularized bone grafts in scaphoid nonunion with avascular necrosis: a canine experimental study. J Hand Surg [Am]. 2000;25:849-859.


