CASE 69


History: A 20-year-old jockey fell off his mount without visible injuries but complaining of epigastric pain.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
E. Splenic artery pseudoaneurysm
2. What is the most common cause of pancreatic injury in adults?
3. What structure must be assessed to determine definitive treatment of pancreatic trauma?
4. What is the most common treatment for this condition?
B. Antibiotics and conservative management
C. Percutaneous drainage of any fluid collections
D. Endoscopic pancreatography and pancreatic duct stenting
ANSWERS
CASE 69
Pancreatic Trauma
1. A, B, and C
2. D
3. D
4. A
References
Gupta A, Stuhlfaut JW, Fleming KW, et al: Blunt trauma of the pancreas and biliary tract: a multimodality imaging approach to diagnosis. Radiographics. 2004;24:1381–1395.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 174.
Comment
The pancreas is not often injured by blunt abdominal trauma. (It is injured in less than 12% of cases of blunt abdominal trauma.) The spleen and liver are much more commonly injured. However, the pancreas extends rather far anteriorly in the abdomen and crosses the spine, and both factors contribute to its risk of injury during blunt trauma. Motor vehicle accidents and deceleration injuries are the leading causes of pancreatic injury in adults, whereas child abuse or sports-related or bicycle injuries more typically produce the damage in children. Penetrating trauma is another common cause of pancreatic injury.
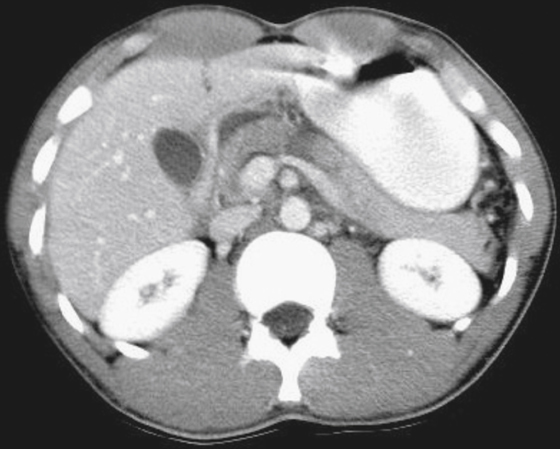
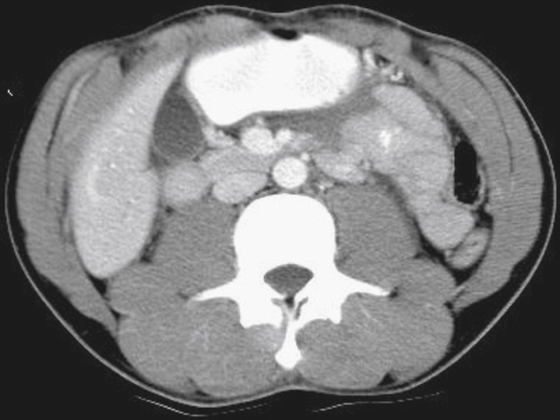
When pancreatic injury occurs, there is a high incidence of associated injuries to the bowel, spleen, liver, and blood vessels. The mortality rate for this injury approaches 20% because of both the pancreatic injury and all the other associated injuries. Patients with pancreatic injury have pain, leukocytosis, and elevated amylase levels. The injury may be just a contusion, a laceration, or a complete transection. The integrity of the pancreatic duct is important; if the duct is compromised or transected, surgical resection is required. For this type of injury, CT is the imaging modality of choice (see figures).
The appearance of the injury can be quite variable. Sometimes little or nothing can be seen. Changes related to pancreatitis, involving fluid, inflammation, or both, can be evident in the region. A contusion can produce a low-density area in the parenchyma or an area of higher density if there is hemorrhage. The actual laceration or tear of the pancreatic tissue may be evident, particularly on high-resolution scans through the pancreas. Surgery is often indicated for patients with this injury to at least drain the peripancreatic tissues of fluid that can accumulate. If the pancreatic duct is injured, the treatment usually requires surgical resection of the pancreas proximal to the injury. Ductal patency might have to be determined by endoscopic retrograde cholangiopancreatography.






