CASE 69
1. What should be included in the differential diagnosis? (Choose all that apply.)
C. Amyloidosis
E. Hypertrophic cardiomyopathy
2. What is the main imaging finding?
A. Ventricular chamber dilation
B. Concentric left ventricular hypertrophy
C. Fatty infiltration of the right ventricular free wall
D. Asymmetric septal hypertrophy
3. What is the most likely diagnosis in a 20-year-old man with sudden cardiac death and no significant past medical history?
A. Arrhythmogenic right ventricular dysplasia
B. Anomalous left coronary artery from the pulmonary artery
C. Obstructing left atrial myxoma
D. Hypertrophic cardiomyopathy
4. What is the mode of inheritance for this condition?
D. X-linked
ANSWERS
Reference
Chun EJ, Choi SI, Jin KN, et al. Hypertrophic cardiomyopathy: assessment with MR imaging and multidetector CT. Radiographics. 2010;30(5):1309–1328.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 88–91.
Comment
Imaging
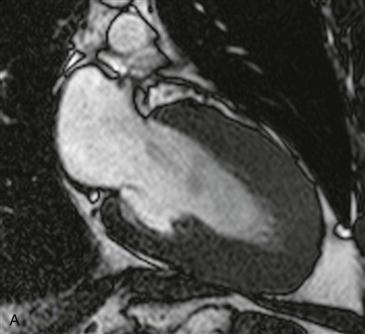
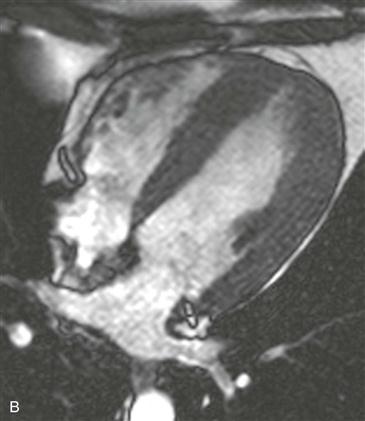
Cine steady-state free precession (SSFP) vertical long-axis and four-chamber views at end-diastole show circumferential left ventricular wall thickening measuring greater than 15 mm in diameter (Figs. A and B). This patient had no systemic condition to explain this degree of wall thickening. The findings are consistent with the concentric or symmetric form of hypertrophic cardiomyopathy.
Criteria for Diagnosis
The maximal left ventricular wall thickness must measure 15 mm or greater in end-diastole to suggest a diagnosis of hypertrophic cardiomyopathy (Figs. A and B). Also, there must be no systemic condition (e.g., hypertension or aortic stenosis) to explain the degree of left ventricular thickening.
Differential Diagnosis
Concentric hypertrophic cardiomyopathy is a less common form of hypertrophic cardiomyopathy. This entity can be diagnosed only after exclusion of other causes of concentric left ventricular wall thickening (e.g., amyloidosis, sarcoidosis, athletic heart, systemic hypertension, and aortic stenosis). MRI is ideally suited to differentiate among the various causes of symmetric left ventricular wall thickening through the use of late gadolinium enhancement and T2-weighted imaging. Amyloidosis is a restrictive cardiomyopathy and characteristically has diffuse subendocardial late gadolinium enhancement. Sarcoidosis causes patchy increased T2 signal and late gadolinium enhancement within portions of the myocardium. Late gadolinium enhancement in sarcoidosis and amyloidosis does not correspond to a vascular territory. Left ventricular wall thickness rarely exceeds 15 mm in patients with aortic stenosis and systemic hypertension, and there is usually no late gadolinium enhancement.