CASE 67
History: A 40-year-old woman presents with intermittent rectal bleeding.
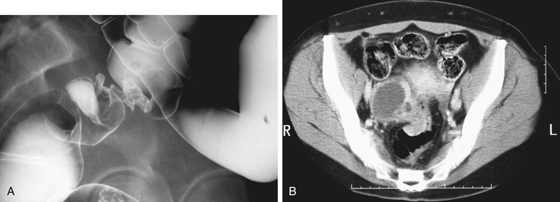
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
B. Peritoneal metastatic cancer
C. Primary gynecologic malignancy
D. Pelvic inflammatory disease
2. If this patient’s symptoms were monthly cyclical, what would be a likely diagnosis?
3. What imaging modalities would be most helpful if endometriosis is suspected?
4. What is the anatomic space anterior to the superior rectum?
ANSWERS
CASE 67
Endometriosis Involving the Rectum
1. A, B, C, and D
2. B
3. B
4. D
References
Jeong YY, Outwater EK, Kang HK. Imaging evaluation of ovarian masses. Radiographics. 2000;20:1445–1470.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 307.
Comment
The anterior wall of the rectum abuts some major structures and can be involved by disease processes arising from these organs. Most important, however, the lowermost portion of the peritoneal cavity, the cul-de-sac, overlies the anterior portion of the upper rectum. Typically this abuts the rectum above the first or second valve of Houston. In this location, any peritoneal process can reside and secondarily involve the rectum.
Inflammatory processes or bleeding from above can result in fluid or pus in the pouch of Douglas (cul-de-sac), but malignancy is the most important factor, and any abdominal tumor can seed the peritoneal cavity with metastatic disease involving the cul-de-sac and the contiguous rectal wall. The most important consideration in a female patient is ovarian carcinoma. Endometrial carcinoma is another possibility. In both sexes, gastric, pancreatic, or colon cancer can produce peritoneal metastases. The appearance of all these tumors is identical.
Inflammatory processes include appendicitis, diverticulitis, and pelvic inflammatory disease. Because the region is the most dependent portion of the peritoneum, all pelvic inflammatory processes can spread to it either before or after surgery.
Endometriosis is a condition produced when there are extrauterine deposits of endometrial tissue. The etiology is uncertain. When endometrial tissue becomes implanted on intra-abdominal structures, it is typically on the ovaries (chocolate cysts) or the serosal surface of the bowel. The tissue is able to maintain viability, and it also responds to the monthly hormonal cycles. The tissue undergoes its normal cyclic changes, including proliferation and then desquamation, just as if it were in the uterine cavity. It is this recurrent shedding of tissue that can lead to complications, including fibrosis. The changes apparent on barium enema relate to fibrotic changes occurring in the wall of the bowel, with some mass effect produced by the tissue (see figures). In addition to the anterior rectum, the sigmoid colon, distal small bowel, cecum, appendix, and other pelvic structures may be involved. Very rarely the condition spreads to the upper abdominal cavity.






