CASE 67

1. What should be included in the differential diagnosis for Figs. A–C? (Choose all that apply.)
A. Sarcoidosis
B. Left ventricle infarction with microvascular obstruction
C. Amyloidosis
D. Left ventricle infarction with thrombus
B. Tumor
D. Myocarditis
3. What is the best imaging clue or test to distinguish a true ventricular aneurysm from a false ventricular aneurysm?
A. Biopsy
B. Location
C. Thrombus
D. Size of neck
4. How is a true aneurysm treated if the patient has refractory arrhythmia?
A. No treatment
ANSWERS
CASE 67
Reference
Kumbasar B, Wu KC, Kamel IR, et al. Left ventricular true aneurysm: diagnosis of myocardial viability shown on MR imaging. AJR Am J Roentgenol. 2002;179(2):472–474.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 235–237.
Comment
Aneurysm Type
Two types of ventricular aneurysm can occur after myocardial infarction—true and false aneurysms. True aneurysms are commonly located at the left ventricular apex or along the left ventricle anteriorly and have wide necks. False aneurysms, or pseudoaneurysms, are commonly located along the left ventricle inferiorly and posteriorly and have narrow necks. Pseudoaneurysms are contained only by pericardium, whereas true aneurysms are contained by infarcted myocardium and pericardium. Distinguishing between these two types of aneurysm is important because treatments differ. True aneurysms have a low likelihood of complications and are generally treated conservatively. False aneurysms have a high rate of rupture and are managed surgically.
Imaging
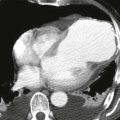
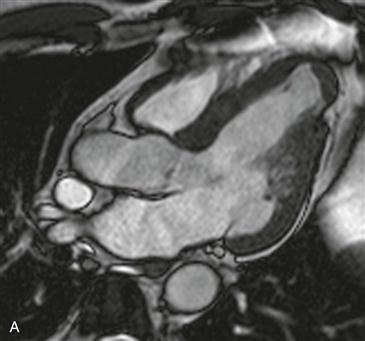
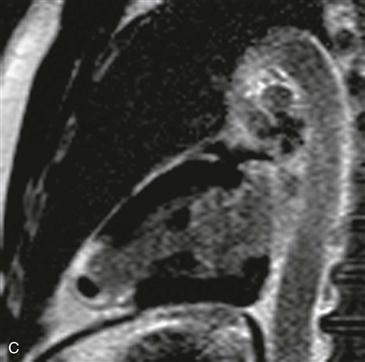
Cine steady-state free precession (SSFP) left ventricular outflow tract view shows a focal outpouching of the left ventricular apex with a wide neck and thinned myocardium (Fig. A). Late gadolinium enhancement four-chamber and vertical long-axis images show circumferential enhancement corresponding to the region of outpouching at the left ventricular apex (Figs. B and C). The adjacent myocardium is of normal thickness and does not enhance. There is an oval-shaped nonenhancing lesion, consistent with thrombus.
Differential Diagnosis
In addition to the location and size of the neck of the aneurysm, late gadolinium enhancement imaging may be useful in differentiating between aneurysm types. As in this case, a true aneurysm is contained by infarcted myocardium and is readily identified by transmural late gadolinium enhancement (Figs. B and C). A false aneurysm has no residual myocardium because it represents a contained ventricular rupture, and its wall does not exhibit late gadolinium enhancement.