CASE 66


History: No patient history is available.
1. Which of the following entities are considered vascular rings or slings? (Choose all that apply.)
A. Left aortic arch with aberrant right subclavian artery
B. Right aortic arch with aberrant left subclavian artery
C. Right aortic arch with mirror image branching
D. Anomalous left pulmonary artery
2. What is the anomaly in this case?
B. Right arch with mirror image branching
C. Right arch with aberrant left subclavian artery
3. What is the most likely clinical presentation in this adult patient?
A. Asymptomatic
C. Hemoptysis
D. Dysphagia
4. What is the most common symptomatic vascular ring?
B. Right aortic arch with aberrant left subclavian artery
ANSWERS
References
Kellenberger CJ. Aortic arch malformations. Pediatr Radiol. 2010;40(6):876–884.
Schlesinger AE, Krishnamurthy R, Sena LM, et al. Incomplete double aortic arch with atresia of the distal left arch: distinctive imaging appearance. AJR Am J Roentgenol. 2005;184(5):1634–1639.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 414–418.
Comment
Epidemiology and Management
Double aortic arch is the most common symptomatic vascular ring. In most cases, the right arch is dominant being higher and larger than the left arch. A double aortic arch compresses and narrows the trachea and esophagus, eventually leading to tracheomalacia with symptoms of dyspnea, wheezing, and dysphagia. Infrequently, a portion of the left arch is atretic. A nonpatent fibrous cord and ductus ligament complete the vascular ring by tethering the atretic left arch to a descending thoracic aortic diverticulum. The fibrous cord and ductus ligament are not seen on imaging, and their positions must be inferred. The goal of cross-sectional imaging is to determine which arch is dominant because this influences surgical management. Treatment is surgical ligation of the smaller arch and ductus ligament via an ipsilateral thoracotomy.
Imaging
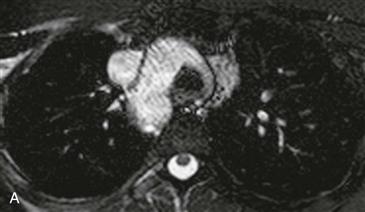
Axial T2-weighted MRI (Fig. A) shows a larger right arch and smaller left arch circumferentially surrounding the upper trachea anteriorly and esophagus posteriorly. Three-dimensional volume-rendered magnetic resonance angiography (MRA) (Fig. B) of the aorta confirms a double aortic arch with the right arch being higher and larger than the left arch. Posterior volume-rendered imaging (Fig. C) shows that the left arch is incomplete and atretic distally at the junction with a descending thoracic aortic diverticulum.
Differential Diagnosis
Differentiation of incomplete double aortic arch with atretic left arch from right aortic arch with mirror image branching is difficult. Imaging clues that favor the former diagnosis include a symmetric appearance of bilateral common carotid and subclavian arteries originating from the right arch and atretic left arch and a diverticulum of the descending thoracic aorta (both present in this case).






