CHAPTER 65 Spinal Anesthesia






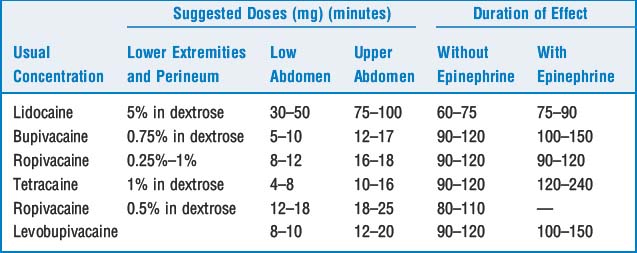
2 What are the usual doses of common local anesthetics used in spinal anesthesia and the duration of effect?
5 Describe the factors involved in distribution (and extent) of conduction blockade
 Patient characteristics include height, position, intra-abdominal pressure, anatomic configuration of the spinal canal, and pregnancy. There is great interindividual variation in lumbosacral CSF volumes; magnetic resonance imaging has shown volumes ranging from 28 to 81 ml. Lumbar CSF volumes correlate well with the height and regression of the block. With the exception of an inverse relation with weight, no external physical measurement reliably estimates lumbar CSF volumes. CSF volumes are also reduced in pregnancy.
Patient characteristics include height, position, intra-abdominal pressure, anatomic configuration of the spinal canal, and pregnancy. There is great interindividual variation in lumbosacral CSF volumes; magnetic resonance imaging has shown volumes ranging from 28 to 81 ml. Lumbar CSF volumes correlate well with the height and regression of the block. With the exception of an inverse relation with weight, no external physical measurement reliably estimates lumbar CSF volumes. CSF volumes are also reduced in pregnancy.


6 At what lumbar levels should a spinal anesthetic be administered? What structures are crossed when performing a spinal block?
8 What are the physiologic changes and risk factors found with subarachnoid block–associated hypotension?
10 Why are patients who have received spinal anesthetics especially sensitive to sedative medications? What is deafferentation?
12 If a patient has a cardiac arrest while having a subarachnoid block, how should resuscitative measures differ from standard advanced cardiac life support protocols?
17 Review the current recommendations for administering regional anesthesia to patients with altered coagulation caused by medications




18 Should spinal (or epidural) anesthesia be performed when unfractionated heparin is administered?




19 Should spinal (or epidural) anesthesia be performed when low-molecular-weight heparin is administered?
 Patients who have received low-molecular-weight heparin (LMWH) should be believed to have altered coagulation, and a single-shot spinal injection is the safest procedure for these patients. As in the case with unfractionated heparin, other factors that increase the likelihood of bleeding will increase the risk of spinal hematoma when LMWH is administered.
Patients who have received low-molecular-weight heparin (LMWH) should be believed to have altered coagulation, and a single-shot spinal injection is the safest procedure for these patients. As in the case with unfractionated heparin, other factors that increase the likelihood of bleeding will increase the risk of spinal hematoma when LMWH is administered.


21 What is transient neurologic syndrome and its cause?
KEY POINTS: Spinal Anesthesia 
1. Loss of afferent sensory and motor stimulation renders a patient sensitive to sedative medications secondary to deafferentation. For the same reason neuraxial anesthesia decreases the minimum alveolar concentration of volatile anesthetics.
2. Vagal predominance suggests that a patient may be at risk for cardiovascular collapse during neuraxial anesthesia.
22 Since lidocaine is associated with TNS, what would be an appropriate local anesthetic selection for an ambulatory procedure?

1. Caplan R.A., Ward R.J., Posner K., et al. Unexpected cardiac arrest during spinal anesthesia: a closed claims analysis of predisposing factors. Anesthesiology. 1988;68:5-11.
2. Zaric D., et al. Transient neurologic symptoms after spinal anesthesia with lidocaine versus other local anesthetics: a systematic review of randomized, controlled trials. Anesth Analg. 2005;100:1811-1816.
3. Hocking G., Wildsmilth J.A.W. Intrathecal drug spread. Br J Anaesth. 2004;93:568-578.
4. Moen V., Dahlgren N., Irestedt L. Severe neurological complications after central neuraxial blockades in Sweden 1990–1999. Anesthesiology. 2004;101:950-959.
