Procedure 65 Arthroscopic Treatment for Septic Arthritis
Indications


Examination/Imaging







Surgical Anatomy



Positioning





Exposures
 Extremity exsanguination is generally contraindicated because of the joint infection. In some situations a tourniquet may be used to allow better visualization of the wrist joint. If a tourniquet is used, the arm is elevated to let the blood drain before tourniquet inflation.
Extremity exsanguination is generally contraindicated because of the joint infection. In some situations a tourniquet may be used to allow better visualization of the wrist joint. If a tourniquet is used, the arm is elevated to let the blood drain before tourniquet inflation.

 The 6R portal is located by palpating the ECU tendon. The portal is made just radial to the tendon.
The 6R portal is located by palpating the ECU tendon. The portal is made just radial to the tendon.
 The 3-4 portal is located by palpating the concavity between the extensor pollicis longus and EDC tendons just distal to Lister tubercle in line with the radial border of the long finger (Fig. 65-2).
The 3-4 portal is located by palpating the concavity between the extensor pollicis longus and EDC tendons just distal to Lister tubercle in line with the radial border of the long finger (Fig. 65-2).


Procedure
Step 1
 Inflow is initially placed through the 6U portal. The joint is inflated.
Inflow is initially placed through the 6U portal. The joint is inflated.

 A blunt curved hemostat should be used to dissect down to the wrist joint capsule using a spread and push technique. Care should be taken to avoid damaging the dorsal sensory nerves and the superficial veins that run in a longitudinal fashion (Fig. 65-3).
A blunt curved hemostat should be used to dissect down to the wrist joint capsule using a spread and push technique. Care should be taken to avoid damaging the dorsal sensory nerves and the superficial veins that run in a longitudinal fashion (Fig. 65-3).

 Entry into the joint capsule should be done in a controlled fashion using gentle pressure on a blunt trocar (Fig. 65-4).
Entry into the joint capsule should be done in a controlled fashion using gentle pressure on a blunt trocar (Fig. 65-4).



Step 1 Pearls
When introducing the blunt trocar, care must be taken not to plunge into the joint space. A controlled entrance is necessary to avoid injury to the internal structures.
The radioscaphocapitate, long radiolunate, triangular fibrocartilage complex, lunotriquetral interosseous ligament, ulnolunate ligament, and ulnotriquetral ligament can all be viewed from the 3-4 portal.
Inflow is provided through the 6U portal and outflow through the arthroscopic cannula. This allows for greater flow of fluid to irrigate the joint (Fig. 65-5).

Step 1 Pitfalls
Inflow through the arthroscope cannula does not provide sufficient irrigation of the joint because of the small space between the arthroscope and the cannula.
Visualization to the synovitis can be initially difficult. Be patient.
Visualization is key. Advance the arthroscope ulnarly near the 6R portal. Insert the shaver and start making room in the joint.
Step 2
 An 18-gauge needle is inserted into the joint under visualization with the arthroscope in the 3-4 portal.
An 18-gauge needle is inserted into the joint under visualization with the arthroscope in the 3-4 portal.



 The 6R portal will be the working portal and will be used for the motorized shaver and suction.
The 6R portal will be the working portal and will be used for the motorized shaver and suction.
Step 3: Radiocarpal Evaluation
 The radiocarpal joint should be examined in a systematic fashion.
The radiocarpal joint should be examined in a systematic fashion.



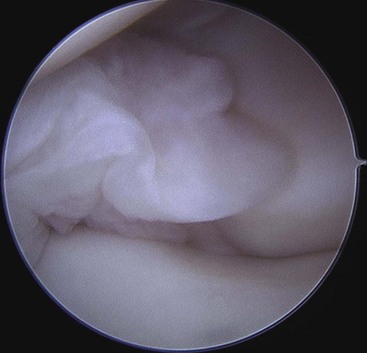
 When synovitis, debris, or loculations are encountered, they should be débrided with the shaver as completely as possible (Fig. 65-6).
When synovitis, debris, or loculations are encountered, they should be débrided with the shaver as completely as possible (Fig. 65-6).


Step 4: Midcarpal Evaluation
 After the proximal radiocarpal joint space has been thoroughly evaluated, the midcarpal space should be examined.
After the proximal radiocarpal joint space has been thoroughly evaluated, the midcarpal space should be examined.


 The distal articular surface of the capitate is easily viewed and should be examined first.
The distal articular surface of the capitate is easily viewed and should be examined first.





Postoperative Care and Expected Outcomes





Birman MV, Strauch RJ. Management of the septic wrist. J Hand Surg [Am]. 2011;36:324-326.
Goldenberg DL, Brandt KD, Cohen AS, Cathcart ES. Treatment of septic arthritis: comparison of needle aspiration and surgery as initial modes of joint drainage. Arthritis Rheum. 1975;18:83-90.
Sammer D, Shin A. Comparison of arthroscopic and open treatment of septic arthritis of the wrist. J Bone Joint Surg [Am]. 2010;92:107-113.


