CHAPTER 64 Pacemakers and Internal Cardioverter Defibrillators
1 Explain the letters in the NBG coding system for pacemakers
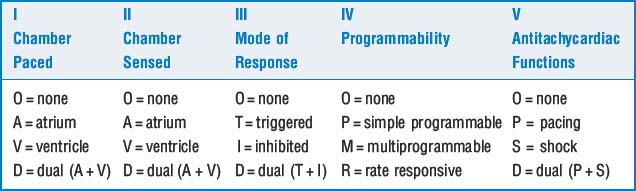
The first three letters refer to chamber paced, chamber sensed, and response to sensed events. The fourth letter generally refers to programmability and rate responsiveness. The fifth letter is rarely used (Table 64-1).
8 What are common indications for permanent pacing?








15 Do typical anesthetics and intraoperative medications affect the ability of implantable cardioverter defibrillators to defibrillate patients?
20 If no underlying rhythm is seen when a pacemaker rate is rapidly decreased, does that mean that the patient is pacemaker dependent?
21 No pacer spikes are seen on the monitoring system with your patient with a pacemaker. Does this mean that the pacemaker is not functioning properly?
22 Does failure of a pacemaker stimulus to capture the heart necessarily imply pacemaker malfunction?
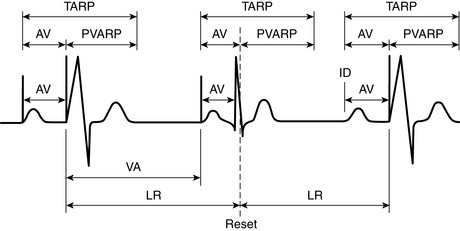
There are many reasons a pacemaker stimulus may not depolarize the tissue. Assess whether a stimulus is an atrial or ventricular stimulus (Figure 64-1). The tissue may have been refractory from a recent event such as a premature ventricular contraction, which is known as functional loss of capture. Occasionally the paced complex is not seen on a single-lead monitoring system because the axis of the paced rhythm is perpendicular to the monitoring lead. In this case the paced complex will not be visible on the lead viewed despite normal function and normal appearance on other leads if they were monitored. However, if repeated failure to capture is seen or the patient appears compromised, emergent evaluation of pacemaker function should be sought.
23 If a pacemaker stimulus is superimposed on a native complex, is the pacemaker necessarily malfunctioning?
No. There are many explanations for the previous finding. Most commonly this is a case in which the pacemaker timer times out before sensing an intrinsic event. In this case the device will release a stimulus. The intrinsic event may have started earlier on a surface lead but was not sensed by the device at the site of the lead until well into the complex. This is a common finding with normal VVI pacing (Figure 64-2). Other programmable behavior may also explain this finding, although inappropriate sensing must also be ruled out.
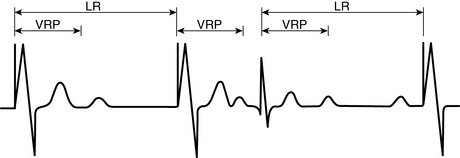
Figure 64-2 Normal VVI pacing.LR is Lower Rate (of pacing), VRP is Ventricular Refractory Period.
(From Zaidan JR: Pacemakers. In Barash PG, editor: Refresher courses in anesthesiology, vol. 21, Philadelphia, 1993, Lippincott, with permission.)
KEY POINTS: Pacemakers and Internal Cardioverter Defibrillators 
1. Ellenbogen K.A., et al. Clinical cardiac pacing, defibrillation, and resynchronization therapy, ed 3. Philadelphia: Saunders, 2007.
2. Hayes D.L., Friedman P.A. Cardiac pacing, defibrillation, and resynchronization: a clinical approach, ed 2. New York: Blackwell Publishing, 2008.
3. Kaszala K., Huizar J.F., Ellenbogen K.A. Contemporary pacemakers: what the primary care physician needs to know. Mayo Clin Proc. 2008;83:1170-1186.
