[level-membership-for-gastroenterology-and-hepatology-category]CASE 64
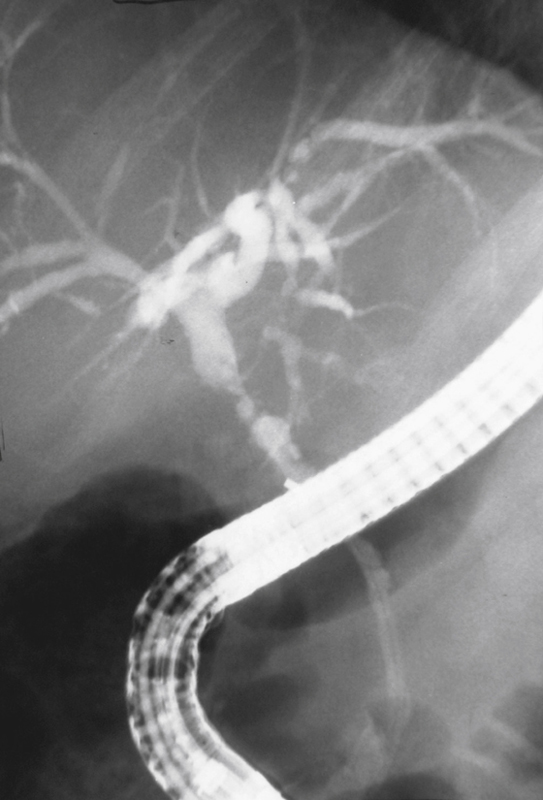
History: A 53-year-old man who had recently undergone cholecystectomy; operative cholangiogram found abnormal bile ducts.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
D. Primary sclerosing cholangitis
E. Recurrent biliary tract infection
2. What is the most common disease associated with sclerosing cholangitis?
3. What is the most common cause of recurrent biliary tract infection worldwide?
4. Which of the following statements regarding malignancy and sclerosing cholangitis is true?
A. Patients are at risk of developing hepatocellular carcinoma.
B. Patients are at risk of developing cholangiocarcinoma.
C. About 50% of patients develop malignant complications.
D. There is no malignant association.
ANSWERS
CASE 64
Sclerosing Cholangitis
1. B, D, and E
2. D
3. D
4. B
References
Chapman R, Fevery J, Kalloo A, et al: Diagnosis and management of primary sclerosing cholangitis. Hepatology. 2010;51:660–678.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 228.
Comment
Primary sclerosing cholangitis is a chronic biliary disease of unknown etiology. The majority (70% or more) of cases are related to underlying inflammatory bowel disease, particularly ulcerative colitis. It is estimated that anywhere from 3% to 10% of patients with ulcerative colitis will develop sclerosing cholangitis. It is a disease of young people (third and fourth decades), with male predominance. Pathologically the condition is caused by multifocal areas of periductal fibrosis, which produce the narrowing, with intervening normal areas developing ductal ectasia (see figure).
Similar radiologic changes are apparent in patients with recurrent biliary tract infections. The groups that typically develop this condition are postoperative patients with complications and the AIDS population. Worldwide, the most likely cause is intestinal parasites, particularly Ascaris lumbricoides. This roundworm migrates into the ducts from the small bowel and causes recurrent cholangitis. The usual course of disease is one of secondary biliary cirrhosis, recurrent sepsis, and eventual hepatic failure. The time between the appearance of the initial symptoms and death is usually 5 to 10 years. Total colectomy (in cases of ulcerative colitis) sometimes halts or diminishes the course of the disease.
Approximately 10% to 20% of patients with sclerosing cholangitis secondary to ulcerative colitis develop cholangiocarcinoma. Interestingly this condition does not develop in patients with Crohn’s disease. Sometimes, total colectomy arrests the liver disease, but this effect is not predictable. If the disease progresses, the only treatment is liver transplantation.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 64
History: A 53-year-old man who had recently undergone cholecystectomy; operative cholangiogram found abnormal bile ducts.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
D. Primary sclerosing cholangitis
E. Recurrent biliary tract infection
2. What is the most common disease associated with sclerosing cholangitis?
3. What is the most common cause of recurrent biliary tract infection worldwide?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
