Procedure 63 Trapeziometacarpal Fusion
 See Video 47: Fusion of Thumb Carpometacarpal Joint
See Video 47: Fusion of Thumb Carpometacarpal Joint
Indications


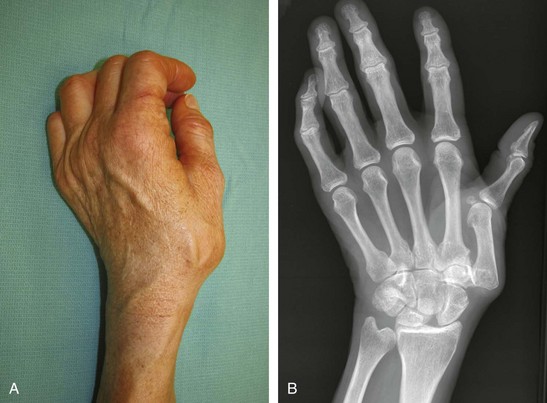
Examination/Imaging





Surgical Anatomy






Exposures
 A 4-cm dorsal longitudinal incision overlying the TMC joint is made in the interval between the extensor pollicis longus (EPL) and EPB tendons to the level of the dorsal joint capsule (Fig. 63-2). The EPL tendon and radial artery should be retracted to expose the joint capsule.
A 4-cm dorsal longitudinal incision overlying the TMC joint is made in the interval between the extensor pollicis longus (EPL) and EPB tendons to the level of the dorsal joint capsule (Fig. 63-2). The EPL tendon and radial artery should be retracted to expose the joint capsule.

Procedure
Step 1


Step 2

Step 3
 A 2.3-mm locking T-plate is applied for arthrodesis. The locking plate is particularly helpful for fusion of this joint because the trapezium may be devoid of strong cortical bone for secure screw purchase in the traditional plating system, which relies on the friction between the screw and the bone for stability. The locking plate system locks the screw to the plate, which adds additional stability to the fusion site. After confirming that the plate is in the center of the metacarpal and that the T portion is centered on the trapezium, a locking screw is placed to secure the plate to the metacarpal. The remaining screws are placed in a locking fashion to provide stable fixation.
A 2.3-mm locking T-plate is applied for arthrodesis. The locking plate is particularly helpful for fusion of this joint because the trapezium may be devoid of strong cortical bone for secure screw purchase in the traditional plating system, which relies on the friction between the screw and the bone for stability. The locking plate system locks the screw to the plate, which adds additional stability to the fusion site. After confirming that the plate is in the center of the metacarpal and that the T portion is centered on the trapezium, a locking screw is placed to secure the plate to the metacarpal. The remaining screws are placed in a locking fashion to provide stable fixation.
Step 4


Step 5
 The periosteal flaps and joint capsule are closed in layers over the implant using 4-0 absorbable braided suture. The tourniquet is released, and all bleeding points are cauterized. Skin is closed using 4-0 permanent monofilament horizontal mattress sutures, and the hand is placed in a thumb spica splint (Fig. 63-5).
The periosteal flaps and joint capsule are closed in layers over the implant using 4-0 absorbable braided suture. The tourniquet is released, and all bleeding points are cauterized. Skin is closed using 4-0 permanent monofilament horizontal mattress sutures, and the hand is placed in a thumb spica splint (Fig. 63-5).

Postoperative Care and Expected Outcomes


Hartigan BJ, Stern PJ, Kiefhaber TR. Thumb carpometacarpal osteoarthritis: arthrodesis compared with ligament reconstruction and tendon interposition. J Bone Joint Surg [Am]. 2001;83:1470-1478.
Kenniston JA, Bozentka DJ. Treatment of advanced carpometacarpal joint disease: arthrodesis. Hand Clin.. 2008;24:285-294.
Taylor EJ, Deari K, D’Arcy JC, Bonnici AV. A comparison of fusion, trapeziectomy and Silastic replacement for the treatment of osteoarthritis of the trapeziometacarpal joint. J Hand Surg [Br]. 2005;30:45-49.


