CHAPTER 63 Sedation and Anesthesia Outside the Operating Room
1 What procedures outside the operating room require sedation or general anesthesia?











2 What equipment and standards are necessary for safely conducting an anesthetic outside the operating room?










3 What monitoring is necessary for administration of any anesthetic, regardless of whether it is in the operating room or elsewhere?




4 How might anesthesiologists be involved in establishing standards for sedation and analgesia conducted by nonanesthesiologists?
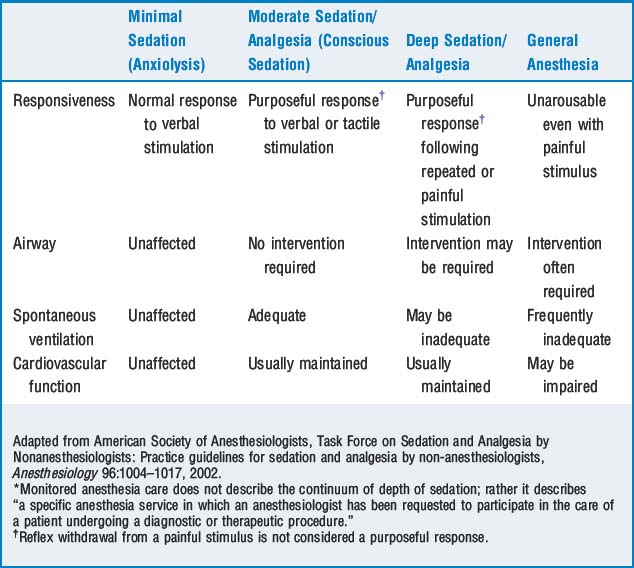
5 Explain conscious sedation and the continuum of depth of anesthesia
The ASA Task Force on Sedation and Analgesia by Nonanesthesiologists states that sedation and analgesia comprise a continuum of states ranging from minimal sedation to general anesthesia. Understanding the concept of the continuum of anesthesia is a critical first step for nonanesthesiologists to administer sedation and analgesia. The term conscious sedation, which is often used by nonanesthesiologists to refer to sedation administered in settings other than the operating room, is considered moderate sedation/analgesia and is defined in Table 63-1.
6 What are some of the requirements for the administration of moderate sedation by nonanesthesiologists?







12 What are some of the more common manifestations of the reactions to soluble contrast media?
| Mild | Moderate | Life-Threatening |
|---|---|---|
| Nausea | Vomiting | Glottic edema/bronchospasm |
| Headache | Rigors | Pulmonary edema |
| Perception of warmth | Feeling faint | Life-threatening arrhythmias |
| Mild urticaria |
13 How is radiation exposure measured?
The roentgen equivalent in humans (rem) is a measure of equivalent dose and relates the absorbed radiation dose in human tissue to the effective biologic damage of the radiation. Equivalent doses are often expressed in terms of thousandths of a rem, or mrem. The Centers for Disease Control and Prevention recommends that the general adult public limit their annual radiation dose to 5000 mrem/year. The equivalent doses from various sources are listed in Table 63-3.
TABLE 63-3 Equivalent Radiation Doses for Medical Procedures
| Medical Procedures | Equivalent Doses |
|---|---|
| Chest x-ray | 8 mrem |
| Extremities x-ray | 1 mrem |
| Dental x-ray | 10 mrem |
| Cervical spine x-ray | 22 mrem |
| Pelvis x-ray | 44 mrem |
| Upper gastrointestinal series | 245 mrem |
| Lower gastrointestinal series | 405 mrem |
| Computed tomography (whole body) | 1100 mrem |
| Background Sources of Radiation | |
| Coast-to-coast airplane roundtrip | 5 mrem |
| Average U.S. cosmic radiation | 27 mrem/year |
| Average U.S. terrestrial radiation | 28 mrem/year |
| Average dose to U.S. public from all sources | 360 mrem/year |
| Recommended Radiation Exposure Limits | |
| Occupational dose limit | 5000 mrem/year |
| Occupational exposure limit for minors | 500 mrem/year |
| Occupational exposure limits for pregnant females | 500 mrem/gestation |
mrem, Roentgen equivalent in humans (in thousandths).
14 How can anesthesiologists protect themselves from radiation exposure?
 Maximize the distance to the source: Newton’s inverse square law, which applies to any point source that spreads its influence in all directions (such as light, sound, gravitational field) tells us that the intensity of the radiation at a given radius is the source strength divided by the sphere area. Or, put more plainly, the intensity (I) of radiation is inversely related to the square of distance (d) from the source:
Maximize the distance to the source: Newton’s inverse square law, which applies to any point source that spreads its influence in all directions (such as light, sound, gravitational field) tells us that the intensity of the radiation at a given radius is the source strength divided by the sphere area. Or, put more plainly, the intensity (I) of radiation is inversely related to the square of distance (d) from the source:

 Minimize the time of exposure: Most medical occupational radiation exposure comes from x-rays scattered by both the patient and surrounding equipment. Obviously this scatter occurs only when the machine is on. A person’s radiation exposure is directly proportional to the length of exposure; thus every reasonable effort to limit the time of exposure is beneficial.
Minimize the time of exposure: Most medical occupational radiation exposure comes from x-rays scattered by both the patient and surrounding equipment. Obviously this scatter occurs only when the machine is on. A person’s radiation exposure is directly proportional to the length of exposure; thus every reasonable effort to limit the time of exposure is beneficial.
15 Define the unique problems associated with providing an anesthetic in the magnetic resonance imaging suite
16 What modifications in the anesthesia machine, ventilator, and monitoring equipment must be made to provide an anesthetic in the magnetic resonance imaging suite?
KEY POINTS: Anesthesia Outside the Operating Room 

1. American Society of Anesthesiologists: Guidelines for nonoperating room anesthetizing locations (last amended on October 15). Park Ridge, Ill.
2. American Society of Anesthesiologists. Task Force on Sedation and Analgesia by Nonanesthesiologists: practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96:1004-1017.
3. Carollo D.S., Nossaman B.D., Ramadhyani U. Dexmedetomidine: a review of clinical applications. Curr Opin Anesthesiol. 2008;21:457-461.
4. Comprehensive Accreditation Manual for Hospitals: The Official Handbook, effective January 2009, Joint Commission on Accreditation of Healthcare Organizations, pp PC 17–18, RC 5–7, RI 5
5. Kotob F., Twersky R.S. Anesthesia outside the operating room: general overview and monitoring standards. Int Anesthesiol Clin. 2003;41:1-15.
6. MacKenzie R.A., Southom P., Stensrud P.E. Anesthesia at remote locations. In: Miller R.D., editor. Anesthesia. ed 5. New York: Churchill Livingstone; 2000:2241-2269.
