[level-membership-for-gastroenterology-and-hepatology-category]CASE 63
History: A 42-year-old man presents with acute right lower quadrant abdominal pain and tenderness.
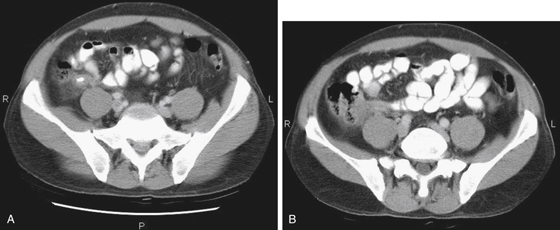
1. Which of the following should be included in the differential diagnosis of the right lower quadrant calcification shown in Figure A? (Choose all that apply.)
2. Which of the following statements regarding appendicoliths is true?
A. An appendicolith is visible in the majority of cases of appendicitis.
B. Appendicitis occurs as a result of an appendicolith obstructing the appendix.
C. The presence of an appendicolith is pathognomonic of appendicitis.
D. They are composed of inspissated fecal debris, mucus, calcium phosphate, and inorganic salts.
3. Which of the following statements regarding appendicitis is true?
A. The optimal management is surgical.
B. The appendix is a considered to be a false diverticulum of the colon.
C. The appendix is a continuation of and histologically similar to the cecum.
D. The primary cause for clinical appendicitis is localized or free perforation of the appendix.
4. Which of the following statements regarding the imaging of appendicitis is true?
A. Appendicitis is diagnosed when CT shows wall thickening more than 10 mm.
B. Ultrasound is useful to diagnose appendicitis in less than 50% of cases.
C. CT has an accuracy rate approaching 100% in the imaging diagnosis of appendicitis.
D. The diagnosis of appendicitis by CT requires the presence of periappendiceal fluid collections.
ANSWERS
CASE 63
Appendocolith with Appendicitis
1. A, B, C, and E
2. D
3. A
4. C
References
Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology. 2000;215:337–348.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 318.
Comment
The advent of multidetector CT scanning (MDCT) in recent years has resulted in an enormous increase in anatomic and pathologic information available to the radiologist, with little change in the radiation dosage to patients. With the improved quality of multiplanar imaging, we are seeing the body with breathtaking clarity compared to previous years. We can now see small calcifications within an otherwise normal appendix. These small calcifications must begin at some time, and it is possible to image the normal appendix with a small appendolith within it. Is it a harbinger of impending appendicitis? That is not known with certainty, but it seems reasonable to assume that these patients are at a higher risk for appendicitis in the future. Currently MDCT has an accuracy rate approaching 100% in the imaging diagnosis of appendicitis. Ultrasound ranges between 70% and 90% in the current literature. Physical examination should be the primary examination of choice, and its role should not be diminished even as imaging becomes more important in the patient work-up. It would be presumptuous to think that everywhere a patient presents with abdominal pain, there will be sophisticated imaging available to make primary diagnosis.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 63
History: A 42-year-old man presents with acute right lower quadrant abdominal pain and tenderness.
1. Which of the following should be included in the differential diagnosis of the right lower quadrant calcification shown in Figure A? (Choose all that apply.)
2. Which of the following statements regarding appendicoliths is true?
A. An appendicolith is visible in the majority of cases of appendicitis.
B. Appendicitis occurs as a result of an appendicolith obstructing the appendix.
C. The presence of an appendicolith is pathognomonic of appendicitis.
D. They are composed of inspissated fecal debris, mucus, calcium phosphate, and inorganic salts.
3. Which of the following statements regarding appendicitis is true?
A. The optimal management is surgical.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
