CASE 62
History: A 45-year-old woman presents with abdominal pain and sepsis.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
D. Xanthogranulomatous pyelonephritis
2. What is the likely state of the bile ducts?
A. Obstructed common hepatic duct
B. Obstructed common bile duct
3. What was the preceding pathology of the condition?
D. Emphysematous cholecystitis
4. Untreated acute cholecystitis can progress to a variety of complications. Which of the following is not a complication of acute cholecystitis?
ANSWERS
CASE 62
Gallbladder Hydrops
1. A, B, C, and E
2. C
3. A
4. D
References
Paulson EK. Acute cholecystitis: CT findings. Semin Ultrasound CT MR. 2000;21:56–63.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 245.
Comment
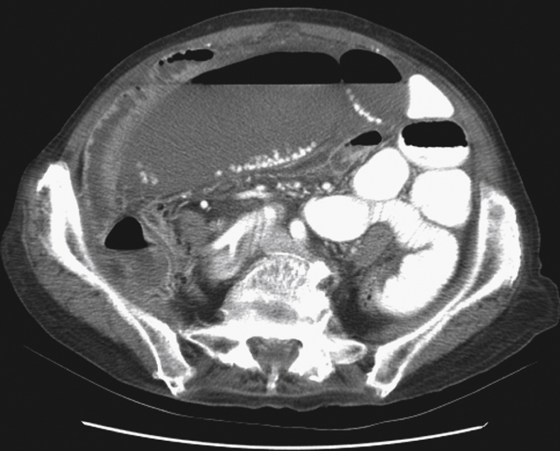
Patients with clinical findings of acute cholecystitis can be imaged either by ultrasound or CT. Ultrasound is very good at making the findings that confirm the diagnosis. However, CT provides additional information about what is happening not only in the right upper quadrant but also throughout the abdomen. In this case, the patient has developed a huge gallbladder (hydrops) with gallstones in the dependent position (see figure) as well as some fluid in the abdomen. Dilated loops of bowel secondary to bile peritonitis are seen nearby. This patient started with a case of acute cholecystitis and, owing to delay in seeking treatment, went on to develop a gangrenous gallbladder wall, perforation, and bile peritonitis.
Chronic cholecystis is relatively common and is seen on many abdominal CT studies, mostly as an incidental finding. Small contracted gallbladder with wall thickening and possibly increased enhancement and occasionally wall calcification are the usual signs. Acute cholecystitis is usually a surgical emergency. CT findings include wall thickening (3 to 4 mm) and wall enhancement. There may be fluid in the gallbladder fossa, and gallstones are usually present. High-resolution CT can often demonstrate the offending stone obstructing the cystic duct. One does have to remember that a small percentage of cases of acute cholecystitis are the acalculous type, with all these findings and no obvious stones.






