[level-membership-for-anesthesiology-category]
CHAPTER 61 High-Risk Obstetrics



2 Describe the hypertensive disorders of pregnancy
Hypertensive disorders occur in approximately 5% to 10% of all pregnancies. Preeclampsia, chronic hypertension, preeclampsia superimposed on chronic hypertension, and gestational hypertension are terms used to describe the hypertensive disorders of pregnancy. The term pregnancy-induced hypertension (PIH) is no longer used (Table 61-1).
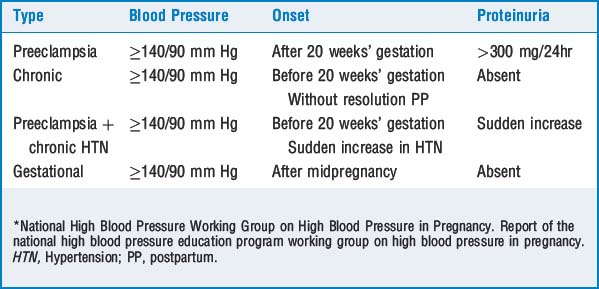
4 What clinical findings are present in preeclampsia?
The principal features of preeclampsia include hypertension and proteinuria. Edema can be physiologic or pathologic and should not be used in the diagnosis of preeclampsia (see Table 61-1).
8 What are the indications for invasive monitoring?




TABLE 61-2 Indications for Invasive Monitoring in Preeclampsia















23 How is congenital heart disease managed during pregnancy?
KEY POINTS: High-Risk Obstetrics 

1. Beilin Y., Reid R.W. Renal disease. In: Chestnut D.H., Polley L.S., Tsen L.C., Wong C.A., editors. Obstetric anesthesia: principles and practice. ed 4. Philadelphia: Elsevier Mosby; 2009:1095-1107.
2. Harnett M., Tsen L.C. Cardiovascular disease. In: Chestnut D.H., Polley L.S., Tsen L.C., Wong C.A., editors. Obstetric anesthesia principles and practice. ed 4. Philadelphia: Elsevier Mosby; 2009:881-912.
3. Mayer D.C., Smith K.A. Antepartum and postpartum hemorrhage. In: Chestnut D.H., Polley L.S., Tsen L.C., Wong C.A., editors. Obstetric anesthesia principles and practice. ed 4. Philadelphia: Elsevier Mosby; 2009:811-836.
4. Polley L.S. Hypertensive disorders. In: Chestnut D.H., Polley L.S., Tsen L.C., Wong C.A., editors. Obstetric anesthesia principles and practice. ed 4. Philadelphia: Elsevier Mosby; 2009:975-1007.
5. Practice Guidelines for obstetric anesthesia: An updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology, 106. 2007:843-863.
6. Practice Guidelines for pulmonary artery catheterization: an updated report by the American Society of Anesthesiologists Task Force on Pulmonary Artery Catheterization. Anesthesiology, 99. 2003:988-1014.
7. Sibai B.M. Hypertension. In: Gabbe S.G., Niebyl J.R., Simpson J.L., editors. Obstetrics: normal and problem pregnancies. ed 5. Philadelphia: Churchill Livingstone; 2007:864-912.
8. Visalyaputra S., Rodanant O., Somboonviboon W., et al. Spinal versus epidural anesthesia for cesarean delivery in severe preeclampsia: a prospective randomized, multicenter study. Anesth Analg. 2005;101:862-868.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 61 High-Risk Obstetrics
2 Describe the hypertensive disorders of pregnancy
Hypertensive disorders occur in approximately 5% to 10% of all pregnancies. Preeclampsia, chronic hypertension, preeclampsia superimposed on chronic hypertension, and gestational hypertension are terms used to describe the hypertensive disorders of pregnancy. The term pregnancy-induced hypertension (PIH) is no longer used (Table 61-1).
4 What clinical findings are present in preeclampsia?
The principal features of preeclampsia include hypertension and proteinuria. Edema can be physiologic or pathologic and should not be used in the diagnosis of preeclampsia (see Table 61-1).
