CASE 60

History: A 54-year-old man presents with right upper quadrant abdominal pain and an episode of jaundice.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
D. Intramural pseudodiverticulosis
E. Cholecystitis glandularis proliferans
2. What is the underlying pathologic process in adenomyomatosis of the gallbladder?
A. Benign glandular tumors derived from biliary tract epithelium
B. Proliferation of the smooth muscle and infolding of the mucosa
C. Granulation and fibrous tissue with plasma cells and lymphocytes
D. Accumulation of lipids within macrophages in the gallbladder wall with enlarged villi
3. What is the long-term complication of adenomyomatosis of the gallbladder?
4. What is the name given to the tiny diverticula-like projections in the thickened gallbladder wall in adenomyomatosis?
D. Intramural pseudodiverticula
ANSWERS
CASE 60
Adenomyomatosis of the Gallbladder
1. A, B, C, and E
2. B
3. D
4. C
References
Berk RN, van der Vegt JH, Lichtenstein JE. The hyperplastic cholecystoses: cholesterolosis and adenomyomatosis. Radiology. 1983;146:593–601.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 252.
Comment
Two conditions—adenomyomatosis and cholesterolosis—are grouped together as the hyperplastic cholecystoses. These conditions are not pathologically or physiologically related in any way, but both produce an abnormal thickening of the gallbladder wall. In adenomyomatosis there is abnormal thickening of the smooth muscle layer of the gallbladder, which results in exaggerated infolding of the mucosal folds and epithelium. Sometimes the epithelium becomes surrounded by the muscle layers and forms cysts. The exact reason that this condition develops is uncertain. Adenomyomatosis is unusual in that often only portions of the gallbladder wall become involved; other gallbladder conditions usually involve the entire gallbladder.
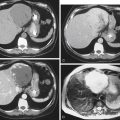
On contrast examinations of the gallbladder, these infoldings of the mucosal surface trap contrast material and appear as tiny diverticula-like projections in the wall (called Rokitansky-Aschoff sinuses). They become particularly pronounced when there is contraction of the gallbladder wall. If the proliferation is severe, there can be narrowing or deformity of the gallbladder lumen (see figure). A thickened gallbladder wall can be demonstrated on CT examination. If this thickening is focal, it can be impossible to distinguish the condition from gallbladder carcinoma. Thickening of the wall of the gallbladder also is apparent on ultrasound examination. Ring-down artifacts may be evident on the nondependent wall of the gallbladder. The wall of the gallbladder also can appear nodular or can appear to contain small polyps. Unlike other gallbladder conditions, there is little associated morbidity with adenomyomatosis, and there are no known long-term complications. Adenomyomatosis is not a precancerous condition.