Procedure 6 Surgical Treatment of de Quervain Tendovaginitis
 See Video 3: Release of First Dorsal Compartment for de Quervain Tendovaginitis
See Video 3: Release of First Dorsal Compartment for de Quervain Tendovaginitis

Examination/Imaging
Clinical Examination
 The patient has tenderness over the radial styloid and may have triggering of the thumb extensor tendons. The following two tests can be done to confirm the presence of de Quervain disease.
The patient has tenderness over the radial styloid and may have triggering of the thumb extensor tendons. The following two tests can be done to confirm the presence of de Quervain disease.




Surgical Anatomy
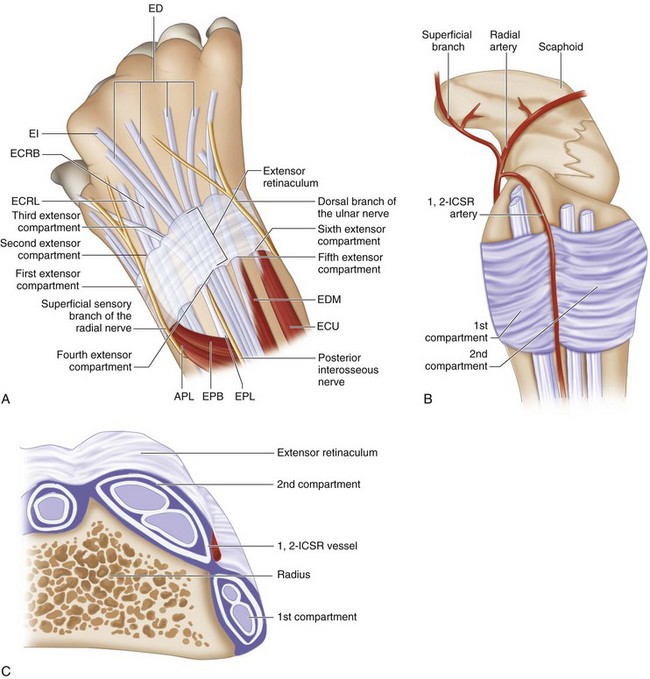
 Six extensor compartments have been described over the dorsum of the wrist (Fig. 6-3A).
Six extensor compartments have been described over the dorsum of the wrist (Fig. 6-3A).
 The first dorsal compartment is involved in de Quervain tendovaginitis. It contains two tendons, the APL and the EBP (Fig. 6-3B and C). The APL tendon has multiple slips. The APL tendon is more radial and volar, whereas the EPB tendon is ulnar and dorsal. In up to 40% of subjects, there may be a separate subsheath for each of the two tendons.
The first dorsal compartment is involved in de Quervain tendovaginitis. It contains two tendons, the APL and the EBP (Fig. 6-3B and C). The APL tendon has multiple slips. The APL tendon is more radial and volar, whereas the EPB tendon is ulnar and dorsal. In up to 40% of subjects, there may be a separate subsheath for each of the two tendons.


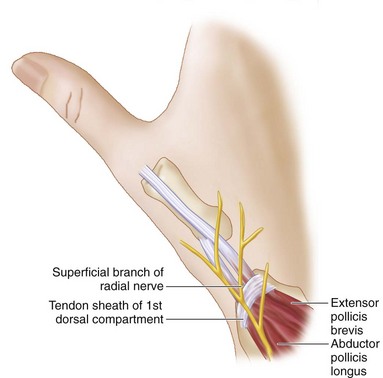
 The radial sensory nerve has several branches in the subcutaneous tissue superficial to the extensor retinaculum. Most complications during this operation are a result of traction injury of this nerve, leading to persistent pain at the incision site (Fig. 6-4).
The radial sensory nerve has several branches in the subcutaneous tissue superficial to the extensor retinaculum. Most complications during this operation are a result of traction injury of this nerve, leading to persistent pain at the incision site (Fig. 6-4).


Exposures
 A 3-cm longitudinal chevron incision is made extending proximally from the radial styloid over the first compartment (Fig. 6-5). As soon as the deep portion of the dermis is opened, gentle blunt dissection with a scissors should be used to expose the extensor retinaculum over the first dorsal compartment. The skin flaps can then be gently elevated to fully expose the first compartment.
A 3-cm longitudinal chevron incision is made extending proximally from the radial styloid over the first compartment (Fig. 6-5). As soon as the deep portion of the dermis is opened, gentle blunt dissection with a scissors should be used to expose the extensor retinaculum over the first dorsal compartment. The skin flaps can then be gently elevated to fully expose the first compartment.

Pearls
The scissors should be spread in a longitudinal direction to avoid injury to the longitudinally oriented branches of the superficial radial nerve.
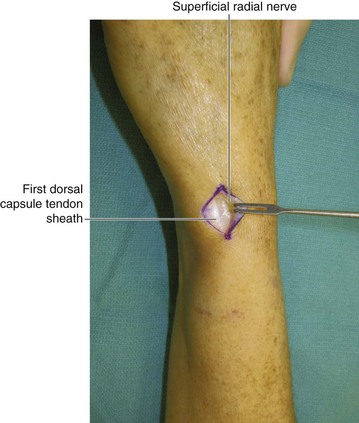
The nerve should be identified and protected. It is best to avoid dissection of the nerve, but where required, a thick cuff of perineural fat should be maintained to prevent adhesions of the nerve to the skin or the scar (Fig. 6-6).
Procedure
Step 1
 The first dorsal compartment is opened along its entire length with a no. 15 scalpel blade (Fig. 6-7). One should inspect the compartment for presence of any subsheaths, which should be individually released (Fig. 6-8).
The first dorsal compartment is opened along its entire length with a no. 15 scalpel blade (Fig. 6-7). One should inspect the compartment for presence of any subsheaths, which should be individually released (Fig. 6-8).
 Any hypertrophic synovium should be excised.
Any hypertrophic synovium should be excised.
 Release is visually confirmed and verified by taking the thumb through a full range of motion (Fig. 6-9).
Release is visually confirmed and verified by taking the thumb through a full range of motion (Fig. 6-9).





Postoperative Care and Expected Outcomes




Ahuja NK, Chung KC. Fritz de Quervain, MD (1868-1940): stenosing tendovaginitis at the radial styloid process. J Hand Surg [Am]. 2004;29:1164-1170.
Ta KT, Eidelman D, Thomson G. Patient satisfaction and outcomes of surgery for de Quervain’s tenosynovitis. J Hand Surg [Am]. 1999;23:1071-1077.
Weiss AC, Akelman E, Tabatabi M. Treatment of de Quervain’s disease. J Hand Surg [Am]. 1994;19:595-598.
Witt J, Pess G, Gelberman RH. Treatment of de Quervain tenosynovitis: a prospective study of the results of injection of steroids and immobilization in a splint. J Bone Joint Surg [Am]. 1991;73:219-222.


