CASE 59
History: A 21-year-old woman presents with weight loss, diarrhea, and abdominal pain.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in figure A? (Choose all that apply.)
2. Which of these findings are features more suggestive of Crohn’s disease of the colon than of ulcerative colitis?
A. Severe anorectal involvement is rare in Crohn’s
B. Granular mucosa in Crohn’s colitis
C. Contiguous and concentric disease in Crohn’s colitis
D. Discontiguous in ulcerative colitis
E. Aphthous ulcers suggest Crohn’s colitis
3. Which of the following statements regarding colonic ulceration is true?
A. Collar button ulcers are typical in Crohn’s disease
B. Aphthous ulceration is pathognomonic of Crohn’s disease
C. Deep ulceration progressing to fistula formation suggests tuberculosis
D. Crohn’s disease is the most common cause of colovesical fistula.
4. Which of the following correctly describes the “cobblestone” sign?
A. Mucosal ulceration with deep linear penetration
B. Deep linear and serpiginous ulceration between lobules of edema
C. Small superficial ulcers with a surrounding slightly elevated mound of edema
ANSWERS
CASE 59
Crohn’s Disease of the Colon
1. A, B, D, and E
2. E
3. C
4. B
References
Horsthuis K, Bipat S, Bennink RJ, Stoker J. Inflammatory bowel disease diagnosed with US, MR, scintigraphy, and CT: meta-analysis of prospective studies. Radiology. 2008;247:64–79.
Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of the art. Radiology. 1997;202:597–610.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 294.
Comment
Several types of ulcers are encountered with inflammation of the colon, and these ulcers can also affect all portions of the gastrointestinal tract because the bowel has only a limited number of ways to respond to inflammation of the mucosa. When ulceration extends through the mucosa and muscularis propria, it reaches the submucosa. The epithelium is relatively resistant, but the submucosa has difficulty containing the inflammatory process. Thus, ulcers tend to spread laterally when they reach the submucosa. With their thin necks and wide bases, the ulcers resemble collar buttons, hence the terminology.
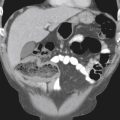
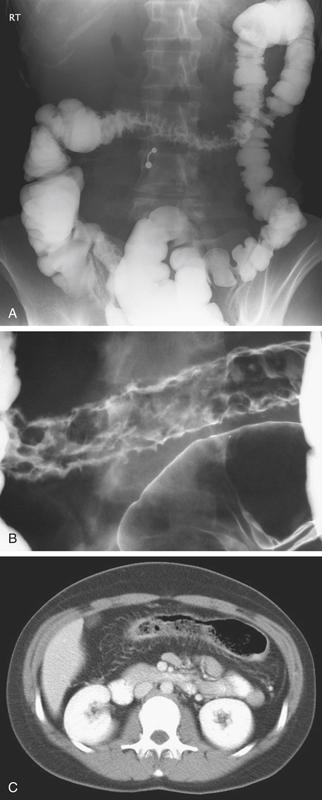
Aphthous ulceration occurs in the colon as lymphoid follicles enlarge from inflammation and their overlying mucosa ulcerates. In other parts of the gastrointestinal tract, aphthous ulcers occur as focal ulcers, with surrounding edema. Either way, they produce a characteristic appearance of a tiny ulcer surrounded by edema (see figures). These ulcers were initially described in association with Crohn’s disease but can be found in a variety of infectious processes, particularly viral infections. Amebiasis, salmonellosis, and even ischemia have also been known to produce aphthous ulcers.
Long, linear ulcers are rare and much more specific to Crohn’s disease. Rarely do other inflammatory conditions cause this type of ulceration, although tuberculosis is also a consideration. Fistulas between bowel loops are a sequela of inflammation of the bowel, occurring with Crohn’s disease or tuberculosis. Fistulas are never seen in patients with ulcerative colitis. The possibility of malignancy and the sequelae of radiation or surgery are other considerations when fistulas are encountered. Diverticulitis also can produce fistulas and is the most common cause of enterovesicular fistulas.
CT is fast becoming a valuable tool in the work-up of Crohn’s disease (see figures). Only about 20% of Crohn’s disease is limited to the colon. The classic findings of discontinuous disease (skip lesions) and asymmetrical involvement are usually evident.