CASE 58

1. What should be included in the differential diagnosis? (Choose all that apply.)
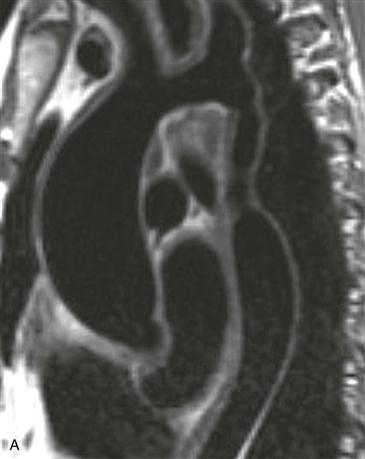
2. Which portion of the aorta is narrowed?
A. Ascending
B. Arch
C. Descending
D. Abdominal
3. What is the most likely diagnosis?
4. Which MRI sequence can be used to quantify collateral circulation?
A. Contrast-enhanced magnetic resonance angiography (MRA)
B. Steady-state free precession (SSFP)
ANSWERS
References
Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184(6):1945–1950.
Hom JJ, Ordovas K, Reddy GP. Velocity-encoded cine MR imaging in aortic coarctation: functional assessment of hemodynamic events. Radiographics. 2008;28(2):407–416.
Reddy GP, Gunn M, Mitsumori LM, et al. Multislice CT and MRI of the thoracic aorta. In: Webb WR, Higgins CB, eds. Thoracic imaging: pulmonary and cardiovascular radiology. ed 2 Philadelphia: Lippincott Williams & Wilkins; 2010.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 393–394.
Comment
Clinical Features
Congenital coarctation is most commonly discrete and juxtaductal in location. Long-segment coarctations may be acquired; Takayasu arteritis is an important cause. Takayasu arteritis (pulseless disease or Martorell syndrome) is an idiopathic disease that is characterized by wall thickening of the aorta and/or arch vessels along with stenosis of the aorta and its branches. Other arteries, such as the pulmonary arteries, can be involved. Patients typically have nonspecific systemic symptoms during the active phase of the disease. In the sclerotic phase, symptoms of vascular insufficiency develop, including abdominal angina and claudication. Hypertension is frequent. The two main large vessel arteritidies include Takayasu and giant cell arteritis which are differentiated by clinical features. Takayasu arteritis most commonly affects women between 10 and 40 years of age, whereas giant cell arteritis occurs in patients older than 50. High-dose corticosteroids are generally the treatment of choice.
Imaging
In Takayasu arteritis, MRI and CT can show stenosis, occlusion, or dilation of the aorta and its branches or a combination of all three. On MRI, the active phase of the disease manifests as wall thickening and enhancement. An aortic wall thickness of greater than 3 mm has been proposed as a marker for early Takayasu arteritis. In the sclerotic phase, MRI can demonstrate areas of stenosis (Figs. A and B) and CT can show concentric aortic wall calcification. Velocity-encoded cine phase contrast imaging can be used to measure collateral circulation. PET is useful for monitoring disease response in patients with large vessel vasculitides. Decreasing FDG activity is considered a favorable response to therapy and may be seen prior to anatomic imaging showing decreased aortic wall thickening.






