[level-membership-for-anesthesiology-category]
CHAPTER 57 Pediatric Anesthesia
1 What are the differences between the adult and pediatric airways?
TABLE 57-1 Differences Between the Adult and Pediatric Airways
| Infant Airway | Significance |
|---|---|
| Obligate nose breathers, narrow nares | Infants can breathe only through their noses, which can become easily obstructed by secretions. |
| Large tongue | May obstruct airway and make laryngoscopy and intubation difficult. |
| Large occiput | Sniffing position achieved with roll under shoulder. |
| Glottis located at C3 in premature babies, C3-C4 in newborns, and C5 in adults | Larynx appears more anterior; cricoid pressure frequently helps with laryngeal visualization. |
| Larynx and trachea are funnel shaped | Narrowest part of the trachea is at the vocal cords; the patient should have an ETT leak of <30 cm H2O to prevent excessive pressure on the tracheal mucosa, barotrauma. |
| Vocal cords slant anteriorly | Insertion of ETT may be more difficult. |
ETT, Endotracheal tube.
2 Are there any differences in the adult and pediatric pulmonary systems?
TABLE 57-2 Differences in the Pediatric and Adult Pulmonary Systems
| Pediatric Pulmonary System | Significance |
|---|---|
| Decreased, smaller alveoli | Thirteenfold growth in number of alveoli between birth and 6 years; threefold growth in size of alveoli between 6 years and adulthood |
| Decreased compliance | Increased likelihood of airway collapse |
| Increased airway resistance, vulnerability to smaller airways | Increased work of breathing and disease affecting small airways |
| Horizontal ribs, pliable ribs and cartilage | Inefficient chest wall mechanics |
| Less type 1, high-oxidative muscle | Babies tire more easily |
| Decreased total lung capacity, faster respiratory and metabolic rate | Quicker desaturation |
| Higher closing volumes | Increased dead-space ventilation |
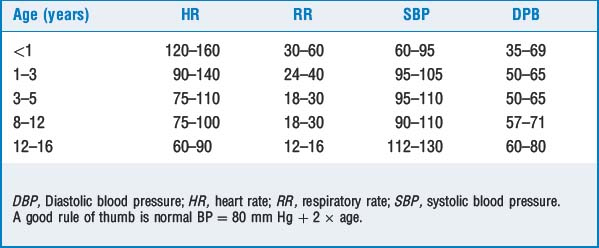
3 How does the cardiovascular system differ in a child?



8 Describe the commonly used induction techniques in children
 Inhalational induction is the most common induction technique in children younger than 10 years who do not have intravenous (IV) access. The child is asked to breathe 70% nitrous oxide (N2O) and 30% oxygen for approximately 1 minute; sevoflurane is then turned on. The sevoflurane concentration can be increased slowly or rapidly.
Inhalational induction is the most common induction technique in children younger than 10 years who do not have intravenous (IV) access. The child is asked to breathe 70% nitrous oxide (N2O) and 30% oxygen for approximately 1 minute; sevoflurane is then turned on. The sevoflurane concentration can be increased slowly or rapidly.


9 How does the presence of a left-to-right shunt affect inhalational induction and intravenous induction?
11 What other special precautions need to be taken in a child with heart disease?
 The anatomy of the lesion(s) and direction of blood flow should be determined. Pulmonary vascular resistance (PVR) needs to be maintained. If the PVR increases, right-to-left shunting may increase and worsen oxygenation, whereas a patient with a left-to-right shunt may develop a reversal in the direction of blood flow (Eisenmenger’s syndrome). If a patient has a left-to-right shunt, decreasing the PVR may increase blood flow to the lungs and lead to pulmonary edema. Decreasing the PVR in patients with a right-to-left shunt may improve hemodynamics. Conditions that can increase shunting are listed in Table 57-5.
The anatomy of the lesion(s) and direction of blood flow should be determined. Pulmonary vascular resistance (PVR) needs to be maintained. If the PVR increases, right-to-left shunting may increase and worsen oxygenation, whereas a patient with a left-to-right shunt may develop a reversal in the direction of blood flow (Eisenmenger’s syndrome). If a patient has a left-to-right shunt, decreasing the PVR may increase blood flow to the lungs and lead to pulmonary edema. Decreasing the PVR in patients with a right-to-left shunt may improve hemodynamics. Conditions that can increase shunting are listed in Table 57-5.



| Left-to-Right Shunt | Right-to-Left Shunt |
|---|---|
| Low hematocrit | Decreased SVR |
| Increased SVR | Increased PVR |
| Decreased PVR | Hypoxia |
| Hyperventilation | Hypercarbia |
| Hypothermia | Acidosis |
| Isoflurane | Nitrous oxide, ketamine |
PVR, Pulmonary vascular resistance; SVR, systemic vascular resistance.
12 How is an endotracheal tube of appropriate size chosen?
An endotracheal tube (ETT) a half size above and a half size below the estimated size in Table 57-6 should be available, the leak around the tube should be <30 cm H2O, and the ETT should be placed to a depth of approximately three times its internal diameter.
| Age | Size—Internal Diameter (mm) |
|---|---|
| Newborns | 3.0–3.5 |
| Newborn–12 months | 3.5–4.0 |
| 12–18 months | 4.0 |
| 2 years | 4.5 |
| >2 years | ETT size = (16 + age)/4 |
ETT, Endotracheal tube.
13 Can cuffed endotracheal tubes be used in children and laryngeal mask airways?
14 How is an appropriate-size laryngeal mask airway chosen?
| Size of Child | LMA Size |
|---|---|
| Neonates up to 5 kg | 1 |
| Infants 5–10 kg | 1½ |
| Children 10–20 kg | 2 |
| Children 20–30 mg | 2½ |
| Children/small adults >30 kg | 3 |
| Children/adults >70 kg | 4 |
| Children/adults >80 kg | 5 |
LMA, Laryngeal mask airway.
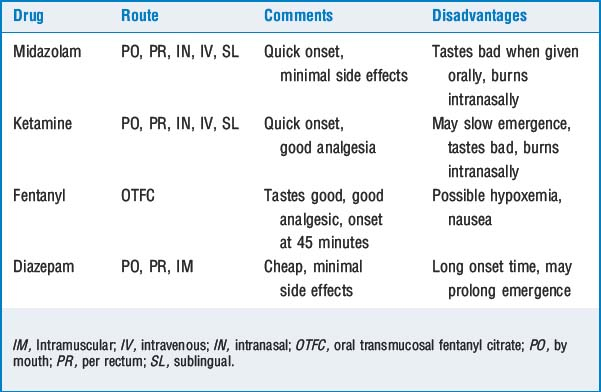
15 How does the pharmacology of commonly used anesthetic drugs differ in children?




16 How is perioperative fluid managed in children?











18 What is the estimated blood volume in children?
TABLE 57-8 Guidelines for Estimated Blood Volume in Children
| Age | EBV (ml/kg) |
|---|---|
| Neonate | 90 |
| Infant up to 1 year old | 80 |
| Older than 1 year | 70 |
EBV, Estimated blood volume.
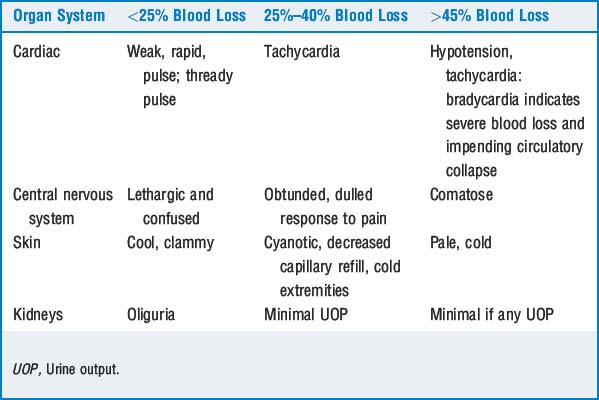
19 How is acceptable blood loss calculated?

where ABL = acceptable blood loss, EBV = estimated blood volume, pt = patient, and hct = hematocrit. The lowest acceptable hematocrit varies with circumstances. Blood transfusion is usually considered when the hematocrit is <21% to 25%. If problems with vital signs develop, blood transfusion may need to be started earlier. For example, a 4-month-old infant is scheduled for craniofacial reconstruction. He is otherwise healthy, and his last oral intake was 6 hours before arriving in the operating room; weight = 6 kg, preoperative hct = 33%, lowest acceptable hct = 25%.




22 What is the most common type of regional anesthesia performed in children? Which local anesthetic is used and what dose is appropriate?
Bupivacaine (0.125% to 0.25%) is most commonly used. Bupivacaine 0.25% produces intraoperative analgesia and decreases the required volatile anesthetic. However, it may produce postoperative motor blockade that interferes with discharge of outpatients. Bupivacaine 0.125% causes minimal postoperative motor block but may not provide intraoperative analgesia or decrease the anesthetic requirements. Bupivacaine 0.175% produces good intraoperative analgesia and minimal motor block and decreases the required MAC of volatile anesthetics. The toxic dose of bupivacaine in the child is 2.5 mg/kg; in the neonate, 1.5 mg/kg. Commonly used doses are listed in Table 57-10.
TABLE 57-10 Commonly used Doses of Local Anesthetic for Caudal Block
| Dose (ml/kg) | Level of Block | Site of Operation |
|---|---|---|
| 0.5 | Sacral/lumbar | Penile, lower extremity |
| 1 | Lumbar/thoracic | Lower abdominal |
| 1.2 | Upper thoracic | Upper abdominal |
UOP, Urine output.
Data from Gunter JB, et al: Optimum concentration of bupivacaine for combined caudal-general anesthesia in pediatric patients, Anesth Analg 66:995–998, 1982.
23 Describe the common postoperative complications
 Postoperative nausea and vomiting (PONV) is the most common cause of delayed discharge or unplanned admission. Factors associated with PONV include age >6 years, length of surgery >20 minutes, previous history of PONV, eye surgery, inner ear procedures, history of motion sickness, tonsillectomy/adenoidectomy, preoperative nausea or anxiety, hypoglycemia, female gender, gynecologic procedures, and use of opioids and N2O. The best treatment for PONV is prevention. Prophylactic administration of an antiemetic should be considered for patients at high risk for PONV. Avoiding opioids decreases the incidence of PONV as long as pain relief is adequate (e.g., patient has a caudal block). Management includes administering IV fluid, limiting oral intake, and administering dexamethasone, metoclopramide, or ondansetron.
Postoperative nausea and vomiting (PONV) is the most common cause of delayed discharge or unplanned admission. Factors associated with PONV include age >6 years, length of surgery >20 minutes, previous history of PONV, eye surgery, inner ear procedures, history of motion sickness, tonsillectomy/adenoidectomy, preoperative nausea or anxiety, hypoglycemia, female gender, gynecologic procedures, and use of opioids and N2O. The best treatment for PONV is prevention. Prophylactic administration of an antiemetic should be considered for patients at high risk for PONV. Avoiding opioids decreases the incidence of PONV as long as pain relief is adequate (e.g., patient has a caudal block). Management includes administering IV fluid, limiting oral intake, and administering dexamethasone, metoclopramide, or ondansetron.

KEY POINTS: Pediatric Anesthesia 
25 Should children with upper respiratory infection receive general anesthesia?
General recommendations for a child with a mild URI include the following:





1. Francis A., Eltaki K., Bash T., et al. The safety of preoperative sedation in children with sleep-disordered breathing. Int J Pediatr Otorhinolaryngol. 2006;70:1517-1521.
2. Goldstein N.A., Pugazhendhi V., Rao S.M., et al. Clinical assessment of pediatric obstructive sleep apnea. Pediatrics. 2004;114:33-43.
3. Gregory G.A. Pediatric anesthesia, ed 4. New York: Churchill Livingstone, 2002.
4. Tait A.R., Malviya S. Anesthesia for the child with an upper respiratory tract infection: still a dilemma? Anesth Analg. 2005;100:59-65.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 57 Pediatric Anesthesia
1 What are the differences between the adult and pediatric airways?
TABLE 57-1 Differences Between the Adult and Pediatric Airways
| Infant Airway | Significance |
|---|---|
| Obligate nose breathers, narrow nares | Infants can breathe only through their noses, which can become easily obstructed by secretions. |
| Large tongue | May obstruct airway and make laryngoscopy and intubation difficult. |
| Large occiput | Sniffing position achieved with roll under shoulder. |
| Glottis located at C3 in premature babies, C3-C4 in newborns, and C5 in adults | Larynx appears more anterior; cricoid pressure frequently helps with laryngeal visualization. |
| Larynx and trachea are funnel shaped | Narrowest part of the trachea is at the vocal cords; the patient should have an ETT leak of <30 cm H2O to prevent excessive pressure on the tracheal mucosa, barotrauma. |
| Vocal cords slant anteriorly | Insertion of ETT may be more difficult. |
ETT, Endotracheal tube.
2 Are there any differences in the adult and pediatric pulmonary systems?
TABLE 57-2 Differences in the Pediatric and Adult Pulmonary Systems
| Pediatric Pulmonary System | Significance |
|---|---|
| Decreased, smaller alveoli | Thirteenfold growth in number of alveoli between birth and 6 years; threefold growth in size of alveoli between 6 years and adulthood |
| Decreased compliance | Increased likelihood of airway collapse |
| Increased airway resistance, vulnerability to smaller airways | Increased work of breathing and disease affecting small airways |
| Horizontal ribs, pliable ribs and cartilage | Inefficient chest wall mechanics |
| Less type 1, high-oxidative muscle | Babies tire more easily |
| Decreased total lung capacity, faster respiratory and metabolic rate | Quicker desaturation |
| Higher closing volumes | Increased dead-space ventilation |
3 How does the cardiovascular system differ in a child?
8 Describe the commonly used induction techniques in children
Inhalational induction is the most common induction technique in children younger than 10 years who do not have intravenous (IV) access. The child is asked to breathe 70% nitrous oxide (N2O) and 30% oxygen for approximately 1 minute; sevoflurane is then turned on. The sevoflurane concentration can be increased slowly or rapidly.9 How does the presence of a left-to-right shunt affect inhalational induction and intravenous induction?
11 What other special precautions need to be taken in a child with heart disease?
The anatomy of the lesion(s) and direction of blood flow should be determined. Pulmonary vascular resistance (PVR) needs to be maintained. If the PVR increases, right-to-left shunting may increase and worsen oxygenation, whereas a patient with a left-to-right shunt may develop a reversal in the direction of blood flow (Eisenmenger’s syndrome). If a patient has a left-to-right shunt, decreasing the PVR may increase blood flow to the lungs and lead to pulmonary edema. Decreasing the PVR in patients with a right-to-left shunt may improve hemodynamics. Conditions that can increase shunting are listed in Table 57-5.[/not-level-membership-for-anesthesiology-category]
