[level-membership-for-gastroenterology-and-hepatology-category]CASE 57


History: A 75-year-old woman presents with a 4-month history of melena, abdominal pain, nausea, and vomiting. Upper endoscopy is unremarkable; colonoscopy revealed diverticular disease only.
1. Which of the following should be included in the differential diagnosis of the imaging findings shown? (Choose all that apply.)
E. Gastrointestinal stromal tumor
2. What is the most common site from where carcinoid tumor arises?
3. What is the substance produced by this lesion that accounts for many of the symptoms?
4. What nonimaging test can be used to confirm the diagnosis?
A. Elevated serum metaiodobenzylguanidine (MIBG) level
B. The presence of vanillylmandelic acid (VMA) in the urine
C. Elevated serum dihydroxyphenylethylamine (dopamine) level
D. The presence of serum vasoactive intestinal polypeptide (VIP)
E. The presence of 5-hydroxindoleacetic acid (5-HIAA) in the urine
ANSWERS
CASE 57
Small Bowel Carcinoid
1. A, B, C, and D
2. A
3. A
4. E
References
Horton KM, Kamel I, Hofmann L, Fishman EK. Carcinoid tumors of the small bowel: a multitechnique imaging approach. Am J Roentgenol. 2004;182:559–567.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 140.
Comment
Carcinoid tumors are unusual neoplasms that can arise in various structures of the intestinal tract and even the bronchi. The most common location in which carcinoids occur is the appendix. However, most symptomatic tumors arise in the small bowel, typically in the ileum. Rarely they are found in other parts of the intestinal tract, the abdominal cavity, and even the bronchi, which is an embryologic bud of the intestinal tract. Carcinoids are slow-growing tumors that invade little by little. They are multiple in about 20% of the cases. All carcinoids are considered premalignant, but those of the small bowel are most likely to metastasize and those of the appendix rarely do so. These tumors belong to the group of lesions termed APUD (amine precursor uptake and decarboxylation) lesions. They are hormonally active, and the major by-product they release is serotonin. Secretion of histamine, 5-hydroxytryptophan, and other hormones also has been described. Serotonin is converted in the liver and lungs to 5-hydroxyindoleacetic acid (5-HIAA), which is excreted in the urine and easily detected.
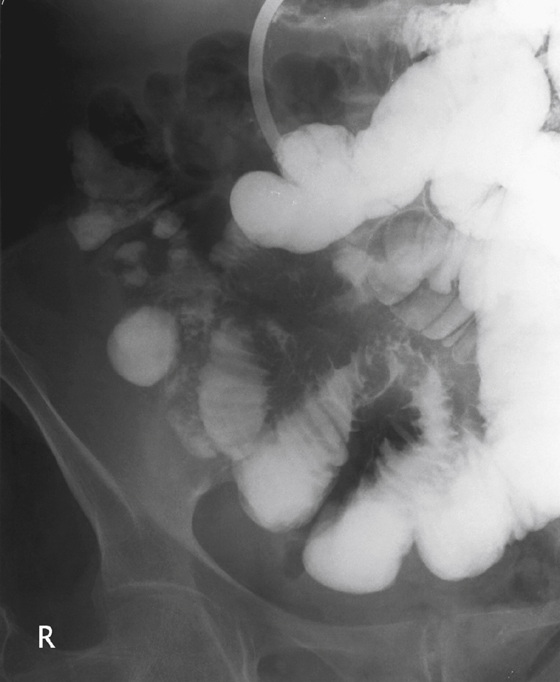
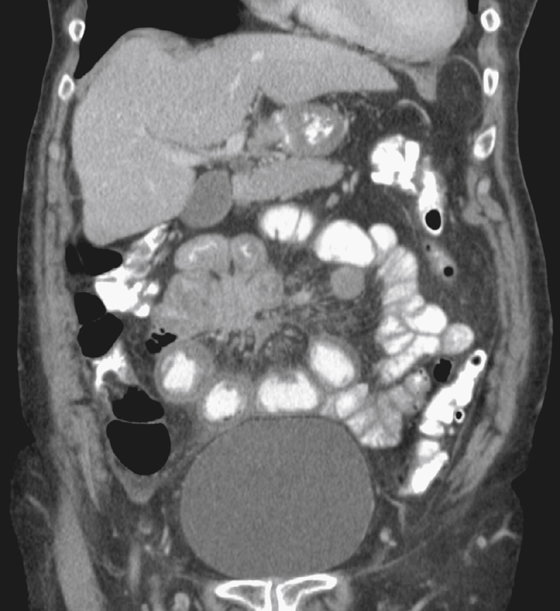
On barium studies of the small bowel the findings are usually irregularity, kinking of the bowel secondary to the desmoplastic nature of the tumor (see figures). This process accounts for the spoke-wheel effect seen on CT (see figures). Also seen in some cases are mass effect and small bowel obstruction (see figures).
Carcinoid syndrome occurs when liver metastases (it rarely occurs without liver metastases) excrete hormonally active substances that cannot be metabolized by the liver directly into a venous circulation. This action produces vasomotor changes of flushing and vasodilation. Bronchospasm and wheezing can occur. Intestinal hypermotility, with diarrhea and cramping, is another symptom. With time, right-sided endocardial fibrosis and valve problems occur in the heart.
The primary tumor can appear as a small mass on conventional barium studies. However the serotonin secreted by the tumor incites an intense desmoplastic response in the mesentery, producing the fibrotic response evident in this patient. There is marked fibrosis of the mesentery, with tethering of the small bowel loops. Bowel obstruction and even vascular obstruction are possible complications of this fibrosis.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 57
History: A 75-year-old woman presents with a 4-month history of melena, abdominal pain, nausea, and vomiting. Upper endoscopy is unremarkable; colonoscopy revealed diverticular disease only.
1. Which of the following should be included in the differential diagnosis of the imaging findings shown? (Choose all that apply.)
E. Gastrointestinal stromal tumor
2. What is the most common site from where carcinoid tumor arises?
3. What is the substance produced by this lesion that accounts for many of the symptoms?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
