Procedure 56 Percutaneous Pinning of Bennett Fracture and Open Reduction and Internal Fixation of Rolando Fracture
Indications
Figures 56-9 through 56-11 provided courtesy of Kevin C. Chung, MD; Figures 56-14 through 56-17 provided courtesy of Sandeep J. Sebastin, MD.
 If the fracture is nondisplaced at initial presentation (uncommon), it can be treated with splint or cast immobilization for 6 weeks, followed by protected motion.
If the fracture is nondisplaced at initial presentation (uncommon), it can be treated with splint or cast immobilization for 6 weeks, followed by protected motion.

 Most Bennett and Rolando fractures are unstable and require surgical intervention.
Most Bennett and Rolando fractures are unstable and require surgical intervention.
 In most cases, closed reduction and percutaneous pinning is indicated for Bennett fractures.
In most cases, closed reduction and percutaneous pinning is indicated for Bennett fractures.






Surgical Anatomy
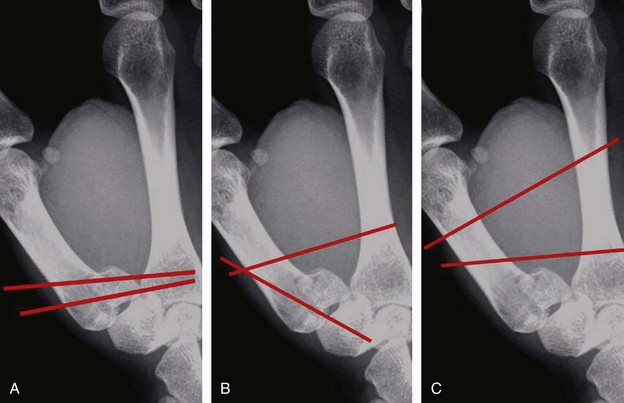
 A Bennett fracture is a two-fragment intra-articular thumb metacarpal base fracture.
A Bennett fracture is a two-fragment intra-articular thumb metacarpal base fracture.
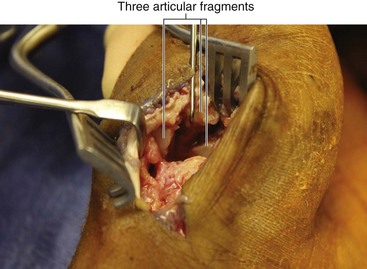
 A Rolando fracture is a three-fragment intra-articular thumb metacarpal base fracture.
A Rolando fracture is a three-fragment intra-articular thumb metacarpal base fracture.




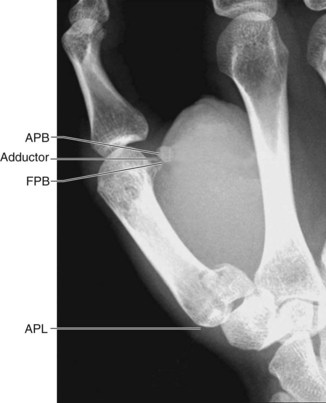
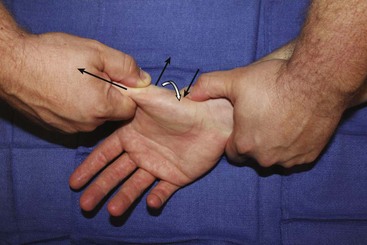
 The abductor pollicis longus (APL) tendon inserts on the dorsal base of the thumb metacarpal and causes dorsal subluxation and proximal displacement of the metacarpal (Fig. 56-1).
The abductor pollicis longus (APL) tendon inserts on the dorsal base of the thumb metacarpal and causes dorsal subluxation and proximal displacement of the metacarpal (Fig. 56-1).
 The adductor pollicis inserts on the metacarpal shaft and causes CMC flexion and adduction (see Fig. 56-1).
The adductor pollicis inserts on the metacarpal shaft and causes CMC flexion and adduction (see Fig. 56-1).

Positioning





Exposures
 If open reduction is required, the exposure is through a modified Wagner incision (Fig. 56-2).
If open reduction is required, the exposure is through a modified Wagner incision (Fig. 56-2).
 The longitudinal limb of the incision is along the glabrous/nonglabrous skin border.
The longitudinal limb of the incision is along the glabrous/nonglabrous skin border.
 At the thumb base, the incision turns ulnarly and extends to the flexor carpi radialis (FCR) tendon.
At the thumb base, the incision turns ulnarly and extends to the flexor carpi radialis (FCR) tendon.
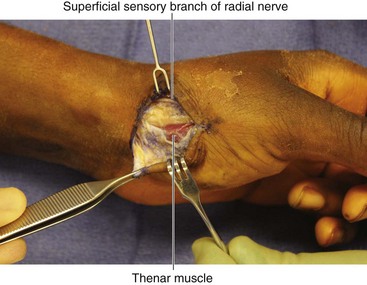
 Dissection is carried down to the border of the thenar musculature, protecting sensory nerve branches in the subcutaneous tissue (Fig. 56-3).
Dissection is carried down to the border of the thenar musculature, protecting sensory nerve branches in the subcutaneous tissue (Fig. 56-3).
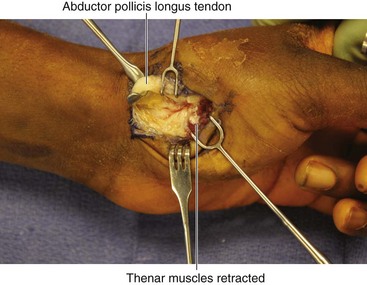
 A no. 15 blade is used to elevate the thenar muscles off of the metacarpal base and trapezium (Fig. 56-4).
A no. 15 blade is used to elevate the thenar muscles off of the metacarpal base and trapezium (Fig. 56-4).
 The APL tendon is reflected ulnarly.
The APL tendon is reflected ulnarly.
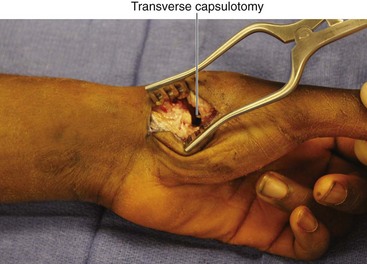
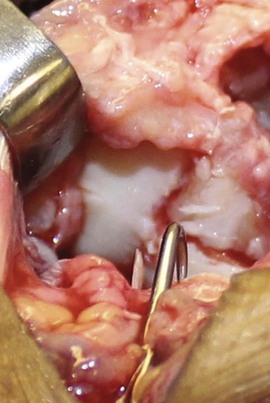
 The joint is then exposed with a transverse capsulotomy, in the interval between the APL and the reflected thenar musculature (Fig. 56-5).
The joint is then exposed with a transverse capsulotomy, in the interval between the APL and the reflected thenar musculature (Fig. 56-5).

Pearls
It is important not to extend the Wagner incision ulnar to the FCR tendon, to avoid injury to the palmar cutaneous branch of the median nerve.
It is important to protect sensory nerves, such as the superficial sensory branches of the radial nerve, and smaller branches of the lateral antebrachial cutaneous nerve (LABC).
Fluoroscopy can be used to confirm joint location before capsulotomy.
Pitfalls
Injury to the palmar cutaneous branch of the median nerve by extending the incision ulnar to the FCR.
Injury to the LABC or superficial sensory branch of the radial nerve.
Excessive soft tissue elevation at the metacarpal base resulting in disinsertion of the APL—care should be taken to preserve the APL insertion.
Procedures
Closed Reduction Percutaneous Pinning of Bennett Fracture
Step 1


Step 2
 While reduction is maintained, K-wires are placed.
While reduction is maintained, K-wires are placed.
 Multiple patterns of K-wire fixation are acceptable (Fig. 56-7); the author’s preference follows.
Multiple patterns of K-wire fixation are acceptable (Fig. 56-7); the author’s preference follows.
Step 2 Pearls
• If placing the initial K-wire while maintaining fracture reduction proves difficult, the K-wire can be placed into the metacarpal base, but not across the fracture, with the fracture unreduced.
• Once the K-wire is in position, the fracture is reduced, and the K-wire is advanced across the fracture and into the Bennett fragment.
• K-wires should be advanced using oscillating mode on the K-wire driver, to avoid injury to sensory nerve branches.
Alternative 1
 A 0.045-inch K-wire is inserted into the thumb metacarpal shaft, beginning at the middle or distal third.
A 0.045-inch K-wire is inserted into the thumb metacarpal shaft, beginning at the middle or distal third.
 It is advanced proximally down the medullary canal and across the CMC joint into the trapezium.
It is advanced proximally down the medullary canal and across the CMC joint into the trapezium.
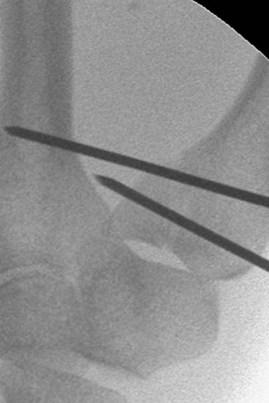
 The leading tip of the K-wire should enter the subchondral bone of the proximal trapezium, without entering the scaphotrapezial joint (Fig. 56-9).
The leading tip of the K-wire should enter the subchondral bone of the proximal trapezium, without entering the scaphotrapezial joint (Fig. 56-9).
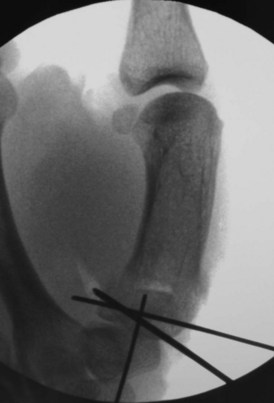
 The second K-wire is then advanced from the radial metacarpal base, across the fracture, and into the Bennett fragment (Fig. 56-10).
The second K-wire is then advanced from the radial metacarpal base, across the fracture, and into the Bennett fragment (Fig. 56-10).
 Alternatively, it can be placed from the thumb metacarpal into the index metacarpal (Fig. 56-11).
Alternatively, it can be placed from the thumb metacarpal into the index metacarpal (Fig. 56-11).












Open Reduction and Percutaneous Pinning of Bennett Fracture



Step 2








Open Reduction and Internal Fixation of Rolando Fracture


Step 2


Step 3










Open Reduction and Percutaneous Pinning of Comminuted Thumb Metacarpal Base Fracture
Step 1




Step 3


Step 4


Step 5






Green DP, O’Brien ET. Fractures of the thumb metacarpal. South Med J. 1972;65:807-814.
Kjaer-Petersen K, Langhoff O, Andersen K. Bennett’s fracture. J Hand Surg [Br]. 1990;15:58-61.
Timmenga EF, Blokhuis TJ, Maas M, et al. Long-term evaluation of Bennett’s fracture: a comparison between open and closed reduction. J Hand Surg [Br]. 1994;19:373-377.



