[level-membership-for-surgery-category]
Procedure 53 Metacarpophalangeal and Proximal Interphalangeal Joint Collateral Ligament Avulsion Fractures
 See Video 39: Metacarpal Shaft Fractures
See Video 39: Metacarpal Shaft Fractures
Indications





Examination/Imaging
Clinical Examination
 Unilateral swelling and bruising of the injured joint
Unilateral swelling and bruising of the injured joint
 Lateral deviation deformity of digit due to loss of collateral ligament integrity (Fig. 53-1)
Lateral deviation deformity of digit due to loss of collateral ligament integrity (Fig. 53-1)
 Pain with restricted range of motion
Pain with restricted range of motion
 Gentle testing of collateral ligaments to ensure integrity, which may require local anesthetic block. Avoid excessive force to prevent displacement of fragment (Fig. 53-2)
Gentle testing of collateral ligaments to ensure integrity, which may require local anesthetic block. Avoid excessive force to prevent displacement of fragment (Fig. 53-2)



Imaging
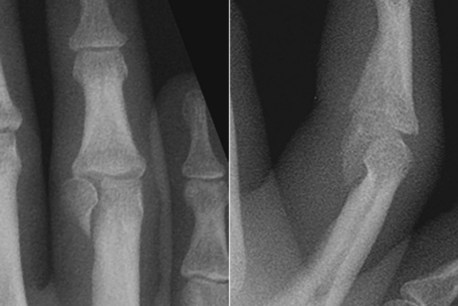
 Posteroanterior, oblique, and true lateral films of the digit for proximal interphalangeal (PIP) joint injuries. At the PIP joint, the most common avulsion fracture is a unicondylar fracture (Fig. 53-3).
Posteroanterior, oblique, and true lateral films of the digit for proximal interphalangeal (PIP) joint injuries. At the PIP joint, the most common avulsion fracture is a unicondylar fracture (Fig. 53-3).
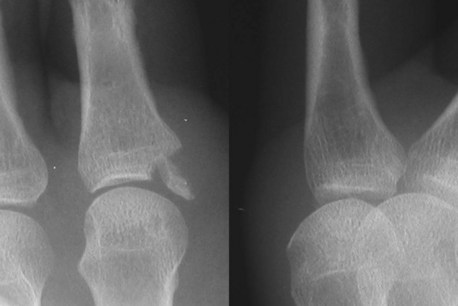
 Posteroanterior, oblique, and true lateral films of the hand for metacarpophalangeal (MCP) joint injuries (Fig. 53-4).
Posteroanterior, oblique, and true lateral films of the hand for metacarpophalangeal (MCP) joint injuries (Fig. 53-4).
 In the immature skeleton, ligament avulsion injuries occur at the growth plate with a fragment of the epiphysis (Fig. 53-5).
In the immature skeleton, ligament avulsion injuries occur at the growth plate with a fragment of the epiphysis (Fig. 53-5).



Surgical Anatomy






Exposures
Metacarpophalangeal Joint
 The MCP joint of the thumb and borders of the hand (ulnar side of small and radial side of index finger) can be easily accessed through a lateral approach.
The MCP joint of the thumb and borders of the hand (ulnar side of small and radial side of index finger) can be easily accessed through a lateral approach.
 Cutaneous nerves are located in the subcutaneous plane and must be identified and preserved.
Cutaneous nerves are located in the subcutaneous plane and must be identified and preserved.



 A Bruner zigzag skin incision is made centered over the proximal digital crease (Fig. 53-6).
A Bruner zigzag skin incision is made centered over the proximal digital crease (Fig. 53-6).
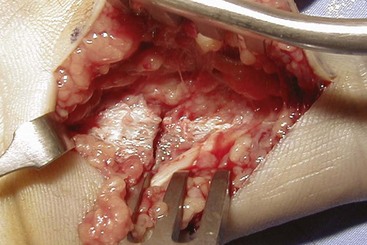
 The flexor sheath is kept intact (Fig. 53-7) and retracted subperiosteally off the base of the proximal phalanx and retracted (Fig. 53-8). After fracture fixation, the sheath is allowed to return to its normal position, and no repair is necessary.
The flexor sheath is kept intact (Fig. 53-7) and retracted subperiosteally off the base of the proximal phalanx and retracted (Fig. 53-8). After fracture fixation, the sheath is allowed to return to its normal position, and no repair is necessary.


Proximal Interphalangeal Joint
 At the PIP level, the fracture is approached using a midaxial incision.
At the PIP level, the fracture is approached using a midaxial incision.
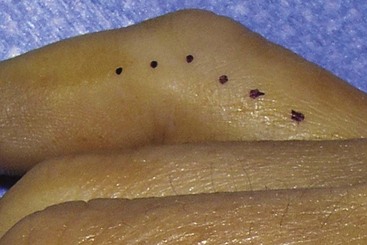
 A digital midaxial incision is marked by joining the most dorsal points of the digital creases with the digit in full flexion (Fig. 53-9).
A digital midaxial incision is marked by joining the most dorsal points of the digital creases with the digit in full flexion (Fig. 53-9).

Pearls
The midaxial skin incision is dorsal to the midlateral line and avoids dissection of the digital neurovascular bundle.
Careful spreading dissection is necessary after skin incision to preserve the subcutaneous nerves.
When exposing the fragments, care must be taken to avoid stripping excessive soft tissue and devascularizing the fragment.
Procedure
Step 1: Principles and Methods of Fixation
 Type of fixation depends on size of fragment and comminution.
Type of fixation depends on size of fragment and comminution.

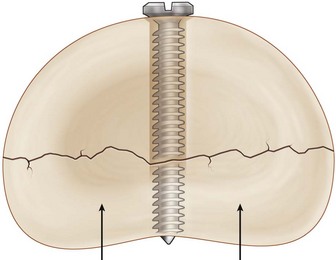
 Lag or compression screw implies a screw that does not have any purchase on the near fragment. This is achieved by drilling a glide hole that exceeds the screw thread diameter in the near cortex. The far cortex is then drilled with the thread hole that matches the screw shaft diameter. As the screw is inserted, it slides through the near cortex and gains purchase in the far cortex. With further tightening, compression between the fragments is generated (Fig. 53-10).
Lag or compression screw implies a screw that does not have any purchase on the near fragment. This is achieved by drilling a glide hole that exceeds the screw thread diameter in the near cortex. The far cortex is then drilled with the thread hole that matches the screw shaft diameter. As the screw is inserted, it slides through the near cortex and gains purchase in the far cortex. With further tightening, compression between the fragments is generated (Fig. 53-10).


Step 1 Pearls
Step 2
 The avulsed fragment is carefully handled to maintain the attached collateral ligament.
The avulsed fragment is carefully handled to maintain the attached collateral ligament.
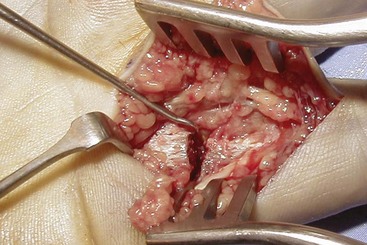
 The fragment must be carefully retracted with a hook, and the joint is subluxated to look for any loose cartilaginous fragments or impaction of the joint surface (Fig. 53-12).
The fragment must be carefully retracted with a hook, and the joint is subluxated to look for any loose cartilaginous fragments or impaction of the joint surface (Fig. 53-12).
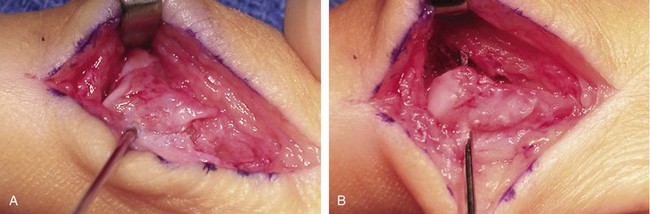
 A 0.035-inch K-wire inserted into the fragment may be used as a joystick to gently manipulate the piece as needed (Fig. 53-13A).
A 0.035-inch K-wire inserted into the fragment may be used as a joystick to gently manipulate the piece as needed (Fig. 53-13A).
 After reduction, the same wire is advanced distally for temporary fixation (Fig. 53-13B).
After reduction, the same wire is advanced distally for temporary fixation (Fig. 53-13B).
 The reduction is then checked by imaging.
The reduction is then checked by imaging.

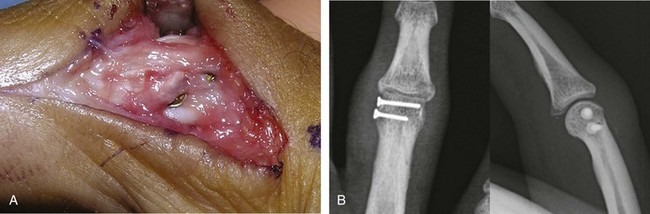
 The K-wire is then removed, and the second screw is inserted through the K-wire hole, after overdrilling the near cortex (Fig. 53-14).
The K-wire is then removed, and the second screw is inserted through the K-wire hole, after overdrilling the near cortex (Fig. 53-14).
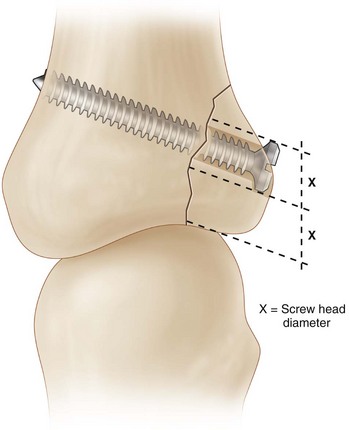
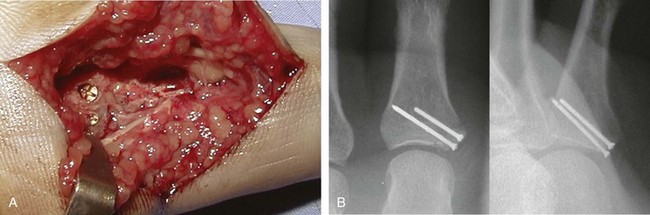
 At the PIP joint, the screw head may interfere with gliding of the near collateral ligament. This can be avoided by placing one screw at or just proximal to the ligament origin. The second screw is placed between the main and accessory parts of the ligament and tightened until it sinks beneath the ligament complex (Fig. 53-15).
At the PIP joint, the screw head may interfere with gliding of the near collateral ligament. This can be avoided by placing one screw at or just proximal to the ligament origin. The second screw is placed between the main and accessory parts of the ligament and tightened until it sinks beneath the ligament complex (Fig. 53-15).
Step 2 Pitfalls
The screw may accidentally penetrate the articular surface.
Placement of a long screw may cause irritation of the extensor mechanism at the base of the proximal phalanx.
A long screw at the head of the proximal phalanx may impinge on the collateral ligament at the far end of the joint and lead to joint stiffness.





Postoperative Care and Expected Outcomes
 The hand is rested in a plaster splint for the first 5 to 7 days after surgery.
The hand is rested in a plaster splint for the first 5 to 7 days after surgery.

 Splinting is discontinued by 4 to 6 weeks when tenderness and swelling have subsided.
Splinting is discontinued by 4 to 6 weeks when tenderness and swelling have subsided.
 Strengthening is commenced after full range of motion has returned.
Strengthening is commenced after full range of motion has returned.


Bischoff R, Buechler U, De Roche R, Jupiter J. Clinical results of tension band fixation of avulsion fractures in the hand. J Hand Surg [Am]. 1994;19:1019-1026.
Kozin SH, Bishop AT. Tension wire fixation of avulsion fractures at the thumb metacarpophalangeal joint. J Hand Surg [Am]. 1994;19:1027-1031.
Schubiner JM, Mass DP. Operation for collateral ligament ruptures of the metacarpophalangeal joints of the fingers. J Bone Joint Surg [Br]. 1989;71:388-389.
Shewring DJ, Thomas RH. Avulsion fractures from the base of the proximal phalanges of the fingers. J Hand Surg [Br]. 2003;28:10-14.
Shewring DJ, Thomas RH. Collateral ligament avulsion fractures from the heads of the metacarpals of the fingers. J Hand Surg [Br]. 2006;31:537-541.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 53 Metacarpophalangeal and Proximal Interphalangeal Joint Collateral Ligament Avulsion Fractures
See Video 39: Metacarpal Shaft Fractures
Indications
Examination/Imaging
Clinical Examination
Unilateral swelling and bruising of the injured joint
Lateral deviation deformity of digit due to loss of collateral ligament integrity (Fig. 53-1)
Pain with restricted range of motion
Gentle testing of collateral ligaments to ensure integrity, which may require local anesthetic block. Avoid excessive force to prevent displacement of fragment (Fig. 53-2)
Imaging
Posteroanterior, oblique, and true lateral films of the digit for proximal interphalangeal (PIP) joint injuries. At the PIP joint, the most common avulsion fracture is a unicondylar fracture (Fig. 53-3).
Posteroanterior, oblique, and true lateral films of the hand for metacarpophalangeal (MCP) joint injuries (Fig. 53-4).
In the immature skeleton, ligament avulsion injuries occur at the growth plate with a fragment of the epiphysis (Fig. 53-5).
Surgical Anatomy
Exposures
Metacarpophalangeal Joint
The MCP joint of the thumb and borders of the hand (ulnar side of small and radial side of index finger) can be easily accessed through a lateral approach.
Cutaneous nerves are located in the subcutaneous plane and must be identified and preserved.
A Bruner zigzag skin incision is made centered over the proximal digital crease (Fig. 53-6).
The flexor sheath is kept intact (Fig. 53-7
[/not-level-membership-for-surgery-category]
