CASE 51

History: A 77-year-old woman with Crohn’s disease and previous jejunal and colorectal resection presents with symptoms that suggest mild active inflammatory disease.
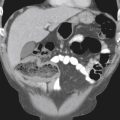
1. Which of the following should be included in the differential diagnosis of the imaging finding in figure A? (Choose all that apply.)
2. This is a spigelian hernia. Through which anatomic area does this hernia pass?
3. What is the unusual type of hernia that contains only a portion of a loop of bowel wall and not the entire lumen?
4. Name the type of hernia that contains Meckel’s diverticulum.
ANSWERS
CASE 51
Ventral Hernia
1. B, C, and E
2. B
3. C
4. A
References
Aguirre DA, Santosa AC, Casola G, Sirlin CB. Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi-detector row CT. Radiographics. 2005;25:1501–1520.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 329.
Comment
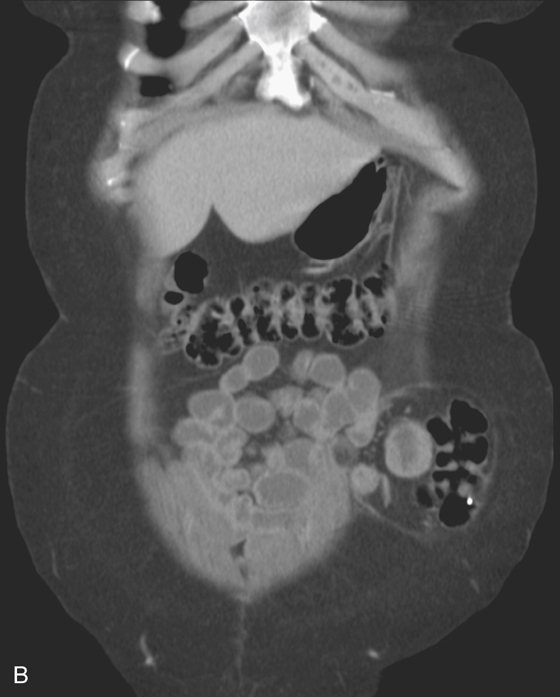
Numerous types of hernias can be identified along the anterior abdominal wall. With the increased use of CT, some hernias are identified in patients who have no symptoms (see figures). In the adult population, incisional hernias are by far the most common. These develop in up to 5% of patients who have abdominal operations and typically occur within the first 6 months after the surgery. Affected patients might remain asymptomatic, however. Even though laparoscopic surgery is becoming increasingly popular, hernias can still occur through those small defects in the abdominal wall because they are not surgically closed. Richter’s hernia is an unusual type of hernia that contains only a portion of a loop of bowel wall and not the entire lumen (e.g., the tip of the cecum caught in a right inguinal hernia).
Spigelian hernias are unusual. They occur in the lower abdomen, either in the right or left lower quadrant. The area through which the bowel herniates, termed the linea semilunaris, consists of a fibrous band of tissue joining the rectus sheath muscles with the transverse abdominal and internal oblique abdominal muscle. The hernia is probably the result of a weakness or congenital defect in the union of these muscles and fibrous bands. The hernia courses obliquely between these groups of muscles and can reside between bands of muscles, making it difficult to identify on clinical examination. Often, patients with spigelian hernias have intermittent or constant pain in the lower quadrant. The hernias contain either small bowel (right) or sigmoid colon (left), depending on where they are situated. They can have a large orifice, in which case there is less likelihood of obstruction or strangulation than with other types of hernias. They also can spontaneously reduce. Because they do not fully herniate through the abdominal wall, they are difficult to clinically diagnose, especially in obese patients. These hernias occur with similar frequency in men and women. They may be bilateral or associated with other abdominal wall defects. Quite often the defect in the abdominal wall contains fat and may be asymptomatic.