Procedure 5 Surgical Treatment of Trigger Digits
 See Video 2: Surgical Treatment of Trigger Digits
See Video 2: Surgical Treatment of Trigger Digits
Indications
 Failure of tendon sheath steroid injections
Failure of tendon sheath steroid injections
 A fixed flexion contracture of the proximal interphalangeal (PIP) joint owing to the triggering
A fixed flexion contracture of the proximal interphalangeal (PIP) joint owing to the triggering



Examination/Imaging
Clinical Examination
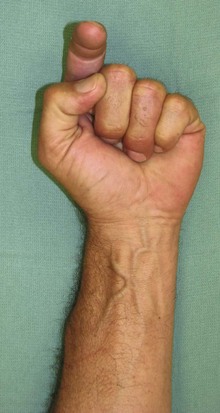
 The patient is examined for a palpable nodule at the level of A1 pulley. The patient may be unable to flex the finger or experience a catching when the finger flexes as the enlarged tendon passes through the A1 pulley (Fig. 5-1).
The patient is examined for a palpable nodule at the level of A1 pulley. The patient may be unable to flex the finger or experience a catching when the finger flexes as the enlarged tendon passes through the A1 pulley (Fig. 5-1).
 The grade of triggering should be recorded for follow-up purposes (Table 5-1). One should look for tenderness over the A1 pulley and a palpable nodule. In long-standing triggering, a flexion contracture of the PIP joint may be present, and the degree of contracture should be noted.
The grade of triggering should be recorded for follow-up purposes (Table 5-1). One should look for tenderness over the A1 pulley and a palpable nodule. In long-standing triggering, a flexion contracture of the PIP joint may be present, and the degree of contracture should be noted.




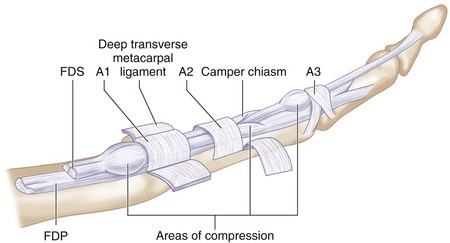
 Congenital trigger finger is a distinct entity related to abnormal thickening of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP), calcifications or granulations within the tendons, or abnormal relationship of the tendons at the FDS decussation. The common sites for triggering in a congenital trigger finger are the A1 pulley, the FDS chiasm, and the A3 pulley (Fig. 5-2).
Congenital trigger finger is a distinct entity related to abnormal thickening of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP), calcifications or granulations within the tendons, or abnormal relationship of the tendons at the FDS decussation. The common sites for triggering in a congenital trigger finger are the A1 pulley, the FDS chiasm, and the A3 pulley (Fig. 5-2).
| Grade I | Before triggering | History of triggering, but not demonstrable on examination |
| Grade II | Active | Demonstrable triggering, but patient can actively overcome the trigger |
| Grade III | Passive | Demonstrable triggering, but patient cannot actively overcome trigger |
| • IIIA | • Extension | • Locked in flexion and needs passive extension to overcome trigger |
| • IIIB | • Flexion | • Locked in extension and needs passive flexion to overcome trigger |
| Grade IV | Contracture | Demonstrable trigger with flexion contracture of posterior interphalangeal joint |

Surgical Anatomy





Exposures
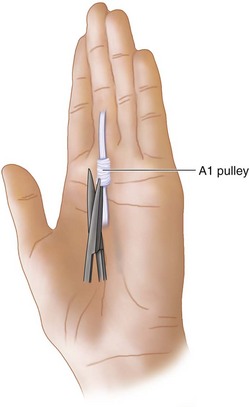
 A 1-cm transverse incision is made in line with the distal palmar crease for the long, ring, and small fingers and at the proximal palmar crease for the index finger (Fig. 5-3).
A 1-cm transverse incision is made in line with the distal palmar crease for the long, ring, and small fingers and at the proximal palmar crease for the index finger (Fig. 5-3).

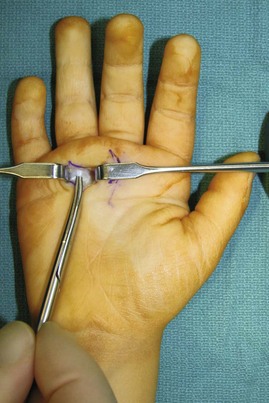
 The subcutaneous fat is gently spread with scissors to expose the tendon sheath and the A1 pulley. Two Ragnell retractors are held by the assistant to maintain visualization (Fig. 5-4).
The subcutaneous fat is gently spread with scissors to expose the tendon sheath and the A1 pulley. Two Ragnell retractors are held by the assistant to maintain visualization (Fig. 5-4).


Pitfalls
Procedure
Primary Trigger Finger Release
Step 1
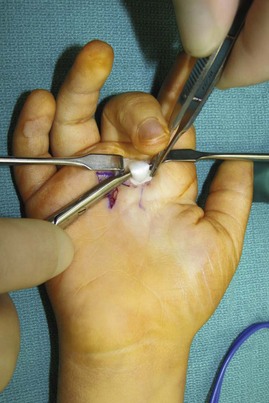
 The A1 pulley is exposed with gentle traction of the soft tissues and incised with a no. 15 blade (Fig. 5-6).
The A1 pulley is exposed with gentle traction of the soft tissues and incised with a no. 15 blade (Fig. 5-6).
 Once identified and partially divided, the scissors is used to complete the sheath division (Fig. 5-7).
Once identified and partially divided, the scissors is used to complete the sheath division (Fig. 5-7).
 Any excessive synovial tissue should also be excised, if encountered.
Any excessive synovial tissue should also be excised, if encountered.


Step 1 Pearls
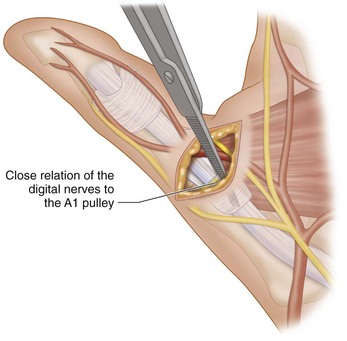
The scissor tips should be placed parallel to the course of the tendon sheath during soft tissue dissection to avoid injury to the neurovascular bundles.
Patients with rheumatoid arthritis and trigger fingers need flexor tenosynovectomy. A1 pulley release may be done only after tenosynovectomy has failed to relieve the trigger. The release of the A1 pulley may contribute to the MCP joint ulnar drift deformity, especially for the index and long fingers, because of the oblique line of pull of the long flexors for these digits. Because of this tendency, some surgeons recommend resection of one slip of the FDS to provide more space for passage of the FDP, as opposed to an A1 pulley release.




Procedure
Congenital Trigger Thumb
Step 1
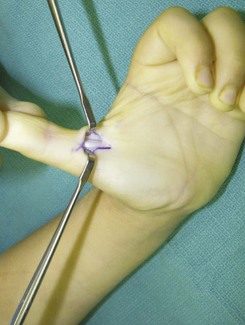
 A longitudinal chevron incision is designed over the metacarpophalangeal joint crease, corresponding to the A1 pulley (Fig. 5-8).
A longitudinal chevron incision is designed over the metacarpophalangeal joint crease, corresponding to the A1 pulley (Fig. 5-8).
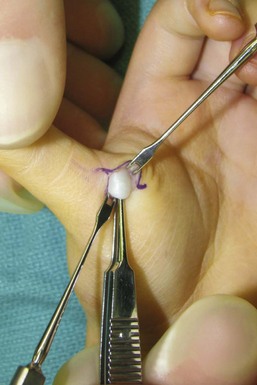
 The A1 pulley and FPL tendon, often with a focal enlargement called the Notta node, are identified using blunt dissection, with care taken to identify and protect the radial digital nerve (Fig. 5-9).
The A1 pulley and FPL tendon, often with a focal enlargement called the Notta node, are identified using blunt dissection, with care taken to identify and protect the radial digital nerve (Fig. 5-9).
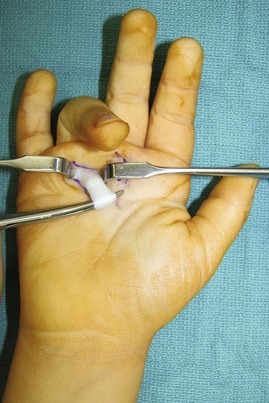
 The A1 pulley is incised with a no. 15 blade, and the remainder of the division is completed with a tenotomy scissors under direct visualization (Fig. 5-10).
The A1 pulley is incised with a no. 15 blade, and the remainder of the division is completed with a tenotomy scissors under direct visualization (Fig. 5-10).





Procedure
Congenital Trigger Finger
 Congenital trigger finger is rare. It is usually due to an enlarged tendon or abnormal anatomic relationship of the FDS and FDP at the FDS decussation. Treatment is directed at specific intraoperative findings but may include not only A1 pulley release but also partial resection of the FDP or FDS tendon.
Congenital trigger finger is rare. It is usually due to an enlarged tendon or abnormal anatomic relationship of the FDS and FDP at the FDS decussation. Treatment is directed at specific intraoperative findings but may include not only A1 pulley release but also partial resection of the FDP or FDS tendon.
Step 1









Bae DS, Sodha S, Waters PM. Surgical treatment of the pediatric trigger finger. J Hand Surg [Am]. 2007;32:1043-1047.
Marks MR, Gunther SF. Efficacy of cortisone injection in treatment of trigger fingers and thumbs. J Hand Surg [Am]. 1989;14:722-727.
Wilhelmi BJ, Snyder N, Verbesey JE, et al. Trigger finger release with hand surface landmark ratios: an anatomic and clinical study. Plast Reconstr Surg. 2001;108:908-915.


