[level-membership-for-gastroenterology-and-hepatology-category]CASE 5
History: A 74-year-old woman presents with left lower quadrant abdominal pain for several days.
1. Which of the following should be included in the differential diagnosis for this patient? (Choose all that apply.)
2. The referring clinician requests further imaging to assist with preoperative planning. Which study is most appropriate?
A. Abdominal and pelvic ultrasound
D. Drainage: CT guided aspiration
3. Which of the following regarding colonic diverticular disease is true?
A. Colonic diverticula are true diverticula.
B. Diverticulitis is the most common cause of colovesical fistula.
C. Diverticular hemorrhage usually ensues if diverticulitis is left untreated.
D. Diverticulitis of the right colon is more likely to progress rapidly to complications.
4. Which of the following regarding the imaging of diverticular disease is true?
A. On plain radiography, the most common appearance is a large bowel obstruction.
B. On barium enema, the appearance of an intramural tract indicates diverticulitis.
C. On CT, the appearance of the inflammatory mass simulates cancer in most cases.
D. Percutaneous abscess drainage is contraindicated if there is large bowel obstruction.
ANSWERS
CASE 5
Sigmoid Diverticulitis
1. C and D
2. B
3. B
4. B
References
Cho KC, Morehouse HT, Alterman DD, Thornhill BA. Sigmoid diverticulitis: diagnostic role of CT comparison with barium enema studies. Radiology. 1990;176:111–115.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 302.
Comment
Diverticular disease of the colon is a very common condition. More than 60% of patients older than 60 years have colonic diverticula, 80% of which occur in the sigmoid segment. Most of these are asymptomatic. Some patients experience recurrent vague abdominal discomfort (spastic bowel), which might represent mild inflammatory changes (preceding frank diverticulitis) around the diverticula.
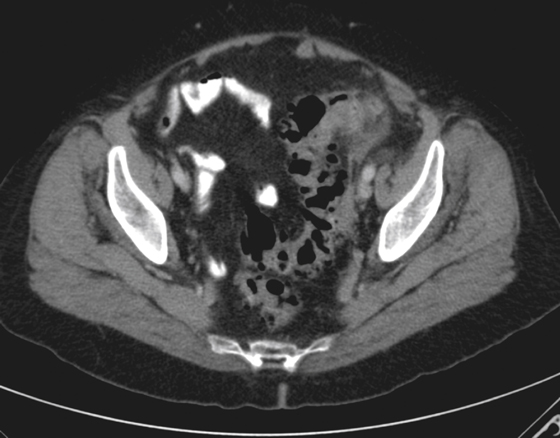
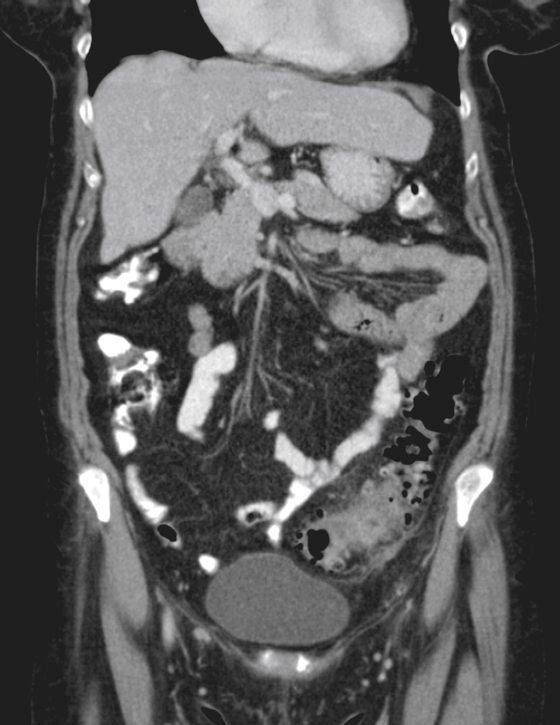
About 5% of the population has diverticulitis. This occurs with perforation of a diverticulum, resulting in intramural and/or localised pericolonic inflammation with all the expected symptoms of diverticulitis: local pain and tenderness, left lower quadrant mass, fever, and leukocytosis.
Plain abdominal radiographs are usually normal. Some patients with diverticulitis present with colonic obstruction. Small bowel obstruction can occur either from localized paralytic ileus or from true obstruction if the small bowel is caught up in the edema or fibrotic scarring surrounding the inflammatory mass.
CT is the modality of choice in acute diverticulitis. It will establish the diagnosis by demonstrating the abnormal segment of colon (colonic wall thickening, presence of diverticula) and the presence of inflammatory changes in the pericolic fat (see figures). Complications such as abscess and fistula formation can be seen.
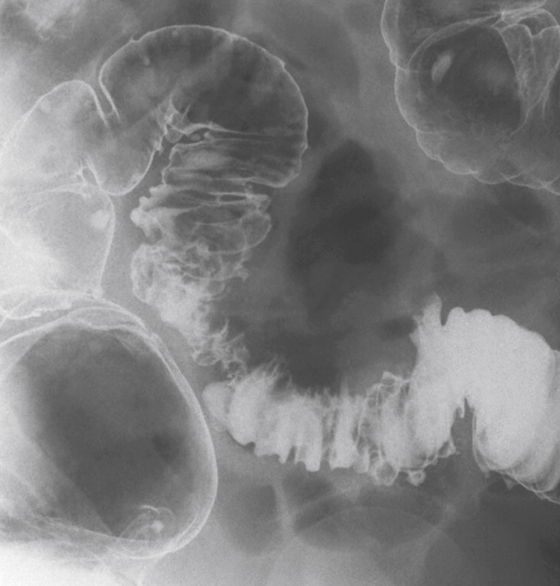
Barium enema is useful in chronic diverticular disease. It is used for operative decision making and planning, to assess the length of colon involved, and to assess the degree of colonic narrowing (see figures).
Some patients experience episodic bleeding. Colonic diverticular hemorrhage is usually painless and occurs unrelated to diverticulitis. The site of bleeding is usually the right colon (75%) owing to the larger neck and dome of these diverticula. The bleeding may be torrential and life threatening.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 5
History: A 74-year-old woman presents with left lower quadrant abdominal pain for several days.
1. Which of the following should be included in the differential diagnosis for this patient? (Choose all that apply.)
2. The referring clinician requests further imaging to assist with preoperative planning. Which study is most appropriate?
A. Abdominal and pelvic ultrasound
D. Drainage: CT guided aspiration
3. Which of the following regarding colonic diverticular disease is true?
A. Colonic diverticula are true diverticula.
B. Diverticulitis is the most common cause of colovesical fistula.
C. Diverticular hemorrhage usually ensues if diverticulitis is left untreated.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
