[level-membership-for-allergy-and-immunology-category]
CASE 5
Bill was apparently well for most of his infant life, although he seemed to both his parents to have had an excess of upper respiratory tract infections and diarrhea (Giardia lamblia) compared with his friends. He had received all childhood immunizations without any notable negative side effects. At the age of 9 he developed an extremely severe case of sinusitis that responded well to antibiotics but caused even his family physician to wonder if there was something else going on. He was small for his age. There were no other siblings, but close attention to the family tree revealed that both an aunt and an uncle had also suffered from recurrent sinopulmonary infections and, in one case, a severe gastrointestinal infection. The aunt was still alive. Unfortunately the uncle had developed leukemia several years earlier and had died unexpectedly while receiving a blood transfusion at a small village hospital where he lived. A cousin had been diagnosed with common variable immunodeficiency (CVID) at age 30. Analysis of serum immunoglobulins using rate nephelometry, a technique that measures the amount of light scatter occurring as a beam of light encounters immune complexes in a dilute solution, showed IgG and IgM levels were normal but IgA levels were not detectable. IgG titers to childhood vaccines were in the normal range. A complete blood cell count with differential showed normal values.
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implication/Analysis of Clinical History
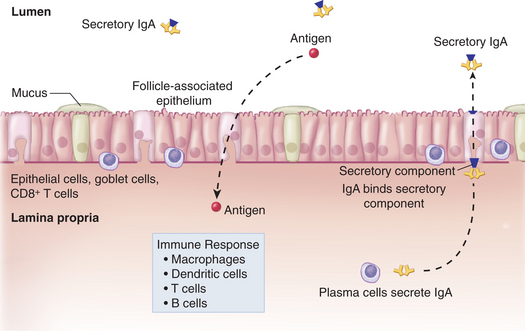
Consider first the types of infections that are reported: upper respiratory tract infections, sinusitis, and giardiasis. All of these infections are occurring in regions lined with mucous membranes where secretory IgA normally has a role in neutralizing pathogens that cause these infections (see Fig. 3-1). Already we should be considering that a defect in IgA is a possibility. This is further supported by the fact that an uncle had died during a blood transfusion (see later). As well, a cousin had been diagnosed with common variable immunodeficiency, a disorder that is more common among relatives of individuals with selective IgA deficiency than one would find in the general population.
THERAPY
Secretory IgA is the predominant antibody at mucosal surfaces; therefore, patients present primarily with sinopulmonary and gastrointestinal infections (Fig. 5-1). In general, it is only necessary to treat the recurrent infections. Any other “heroic” measure to replace missing IgA is not warranted (cost/safety issues). Insufflation (intranasal) IgA preparations have been considered as therapy for upper respiratory tract sinus infections.
ETIOLOGY: SELECTIVE IgA DEFICIENCY
[/level-membership-for-allergy-and-immunology-category][not-level-membership-for-allergy-and-immunology-category]
CASE 5
Bill was apparently well for most of his infant life, although he seemed to both his parents to have had an excess of upper respiratory tract infections and diarrhea (Giardia lamblia) compared with his friends. He had received all childhood immunizations without any notable negative side effects. At the age of 9 he developed an extremely severe case of sinusitis that responded well to antibiotics but caused even his family physician to wonder if there was something else going on. He was small for his age. There were no other siblings, but close attention to the family tree revealed that both an aunt and an uncle had also suffered from recurrent sinopulmonary infections and, in one case, a severe gastrointestinal infection. The aunt was still alive. Unfortunately the uncle had developed leukemia several years earlier and had died unexpectedly while receiving a blood transfusion at a small village hospital where he lived. A cousin had been diagnosed with common variable immunodeficiency (CVID) at age 30. Analysis of serum immunoglobulins using rate nephelometry, a technique that measures the amount of light scatter occurring as a beam of light encounters immune complexes in a dilute solution, showed IgG and IgM levels were normal but IgA levels were not detectable. IgG titers to childhood vaccines were in the normal range. A complete blood cell count with differential showed normal values.
