CASE 46

History: The patient is tall and thin.
1. What are some etiologies for this appearance? (Choose all that apply.)
C. Syphilis
2. What is the most likely diagnosis?
C. Syphilis
3. Which is the pathology of the aortic wall?
C. Arteritis
4. What can be done to reduce the artifact resulting in the undulation of the anterior aortic wall seen in Fig. B?
B. Dual energy
ANSWERS
Reference
Reddy GP, Gunn M, Mitsumori LM, et al. Multislice CT and MRI of the thoracic aorta. In: Webb WR, Higgins CB, eds. Thoracic Imaging: Pulmonary and Cardiovascular Radiology. ed 2 Philadelphia: Lippincott Williams & Wilkins; 2010.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 388–389.
Comment
Pathology and Etiology
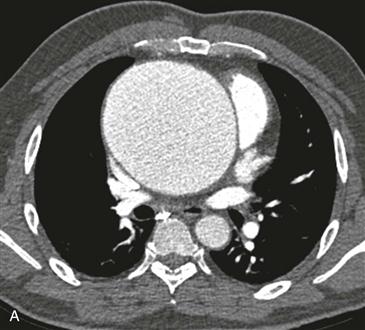
Enlargement of the aortic root and ascending aorta is characteristic of annuloaortic ectasia. The dilation of the aorta in this condition may stop at the sinotubular junction or extend to involve the entire ascending aorta, which is sometimes called the “tulip bulb” configuration. Annuloaortic ectasia results from cystic medial necrosis, which can be idiopathic or can be associated with Marfan syndrome or Ehlers-Danlos syndrome. Progression of annuloaortic ectasia in Marfan syndrome is generally more rapid than the idiopathic variant.
Complications
Complications of annuloaortic ectasia include aortic dissection, aortic rupture, and aortic regurgitation. Although 5.5 to 6 cm is the usual threshold of aortic diameter that necessitates surgery, operative repair may be indicated in annuloaortic ectasia when the aorta reaches a diameter of 5 cm or enlarges rapidly owing to the high risk of rupture.
Imaging
MRI and CT (Figs. A and B) are the most appropriate techniques for imaging of annuloaortic ectasia. MRI has the advantages of no ionizing radiation and the capability to provide quantitative assessment of aortic regurgitation.
Differential Diagnosis
Atherosclerosis is the leading cause of thoracic aortic aneurysms. Most atherosclerotic aneurysms occur in the descending thoracic aorta and commonly coexist with abdominal aortic aneurysms. Syphilis may cause ascending aortic aneurysms, but in contrast to annuloaortic ectasia, there is generally asymmetric involvement or no involvement of the sinuses of Valsalva and aortic root. Noninfectious arteritides (e.g., Takayasu arteritis, rheumatoid arthritis, giant cell arteritis) may cause thoracic aortic aneurysms. There is often circumferential aortic wall thickening with enhancement.






