[level-membership-for-surgery-category]
Procedure 44 Dorsal Metacarpal Artery Perforator Flap
 See Video 36: Dorsal Metacarpal Artery Perforator Flap
See Video 36: Dorsal Metacarpal Artery Perforator Flap
Indications




Examination/Imaging
Clinical Examination





Surgical Anatomy
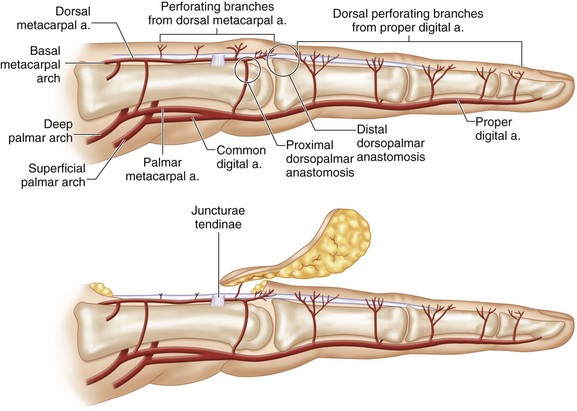
 Vascular basis: The flap is based on the distal cutaneous perforator of the DMA that arises at the level of the metacarpal neck in the second to fourth intermetacarpal spaces. In addition to the DMA, this flap is also nourished by the palmar arterial system through a dorsopalmar anastomosis. This anastomosis is formed by the dorsal perforating branch of the palmar metacarpal artery (arising from the deep palmar arch) and the DMA at the neck of the metacarpal (Fig. 44-2).
Vascular basis: The flap is based on the distal cutaneous perforator of the DMA that arises at the level of the metacarpal neck in the second to fourth intermetacarpal spaces. In addition to the DMA, this flap is also nourished by the palmar arterial system through a dorsopalmar anastomosis. This anastomosis is formed by the dorsal perforating branch of the palmar metacarpal artery (arising from the deep palmar arch) and the DMA at the neck of the metacarpal (Fig. 44-2).
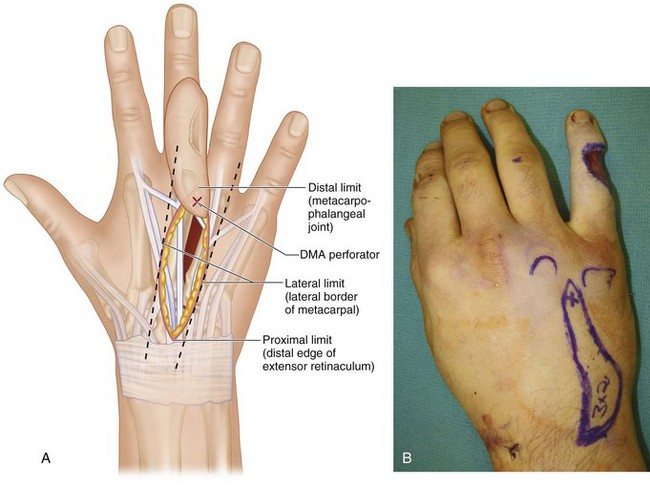
 Limits of the flap: We limit our flaps between the distal edge of the extensor retinaculum, the metacarpophalangeal (MCP) joint, and the outer borders of the adjoining metacarpals (Fig. 44-3A and B).
Limits of the flap: We limit our flaps between the distal edge of the extensor retinaculum, the metacarpophalangeal (MCP) joint, and the outer borders of the adjoining metacarpals (Fig. 44-3A and B).


Exposures
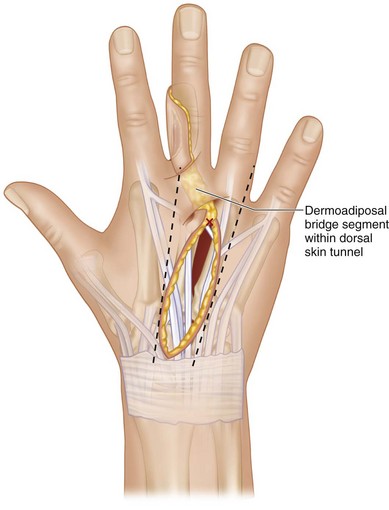
 Flap design: The DMA perforator closest to the defect is marked at the level of the metacarpal neck in the intermetacarpal space. The location of the perforator represents the pivot point of the flap. The distance between the perforator and the proximal edge of the defect represents the bridge segment of the flap. Based on the size of the soft tissue defect, a flap is designed proximal to the perforator at a distance that equals the bridge segment.
Flap design: The DMA perforator closest to the defect is marked at the level of the metacarpal neck in the intermetacarpal space. The location of the perforator represents the pivot point of the flap. The distance between the perforator and the proximal edge of the defect represents the bridge segment of the flap. Based on the size of the soft tissue defect, a flap is designed proximal to the perforator at a distance that equals the bridge segment.

 Flaps with a dermoadiposal bridge segment can reach the defect by passing the bridge under a skin tunnel or by laying open the intervening skin segment (Fig. 44-4).
Flaps with a dermoadiposal bridge segment can reach the defect by passing the bridge under a skin tunnel or by laying open the intervening skin segment (Fig. 44-4).
Pearls
We design the skin island in an oblique fashion when a wider flap is required to accommodate a defect that involves two surfaces (palmar + lateral or dorsal + lateral).
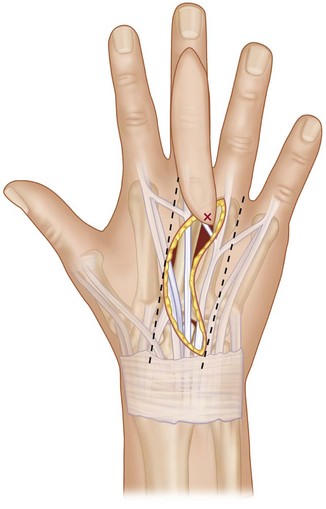
If the flap design extends proximal to the distal edge of the extensor retinaculum, we design the flap as a curved ellipse instead of a straight ellipse. Once the flap is raised, the curved ellipse is straightened out and inset as a straight ellipse. This results in an additional 8 to 10 mm while maintaining the design within the previously mentioned limits (Fig. 44-5).
Procedure
Step 1
 The skin and subcutaneous tissue on one lateral border of the flap are incised until the underlying extensor tendon is seen (Fig. 44-6).
The skin and subcutaneous tissue on one lateral border of the flap are incised until the underlying extensor tendon is seen (Fig. 44-6).

Step 3
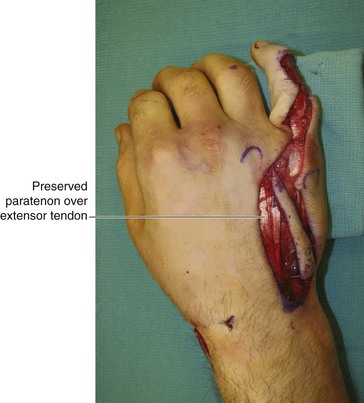
 The remaining lateral border of the flap is incised, and the flap is elevated from proximal to distal (Fig. 44-7).
The remaining lateral border of the flap is incised, and the flap is elevated from proximal to distal (Fig. 44-7).
Step 4
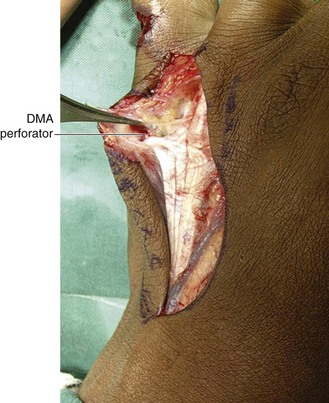
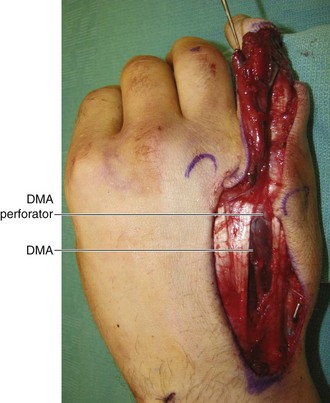
 The DMA perforator is identified, and the flap is incised into an island distal to the perforator (Fig. 44-8).
The DMA perforator is identified, and the flap is incised into an island distal to the perforator (Fig. 44-8).
Step 5
 Any intervening normal skin between the flap and defect can be laid open, or a wide tunnel can be made under it to enable the flap to reach the defect (see Fig. 44-7).
Any intervening normal skin between the flap and defect can be laid open, or a wide tunnel can be made under it to enable the flap to reach the defect (see Fig. 44-7).
Step 5 Pearls
We prefer a tunnel for dorsal defects because the lax dorsal skin permits creation of large tunnels. In addition, this preserves the pliable skin over the dorsum of the MCP joint. For palmar defects, we prefer to lay the tunnel open or use a cutaneous bridge segment because making a tunnel in the palmar skin is difficult, and the constrictive fibrous septae can compromise flap vascularity.
Step 6
 The tourniquet is released with the flap in its native position, and the flap is allowed to perfuse for 10 to 15 minutes. This time is used to achieve excellent hemostasis.
The tourniquet is released with the flap in its native position, and the flap is allowed to perfuse for 10 to 15 minutes. This time is used to achieve excellent hemostasis.
Step 6 Pearls
This flap is now dependent only on the perforating vessel for blood supply. Allowing it to perfuse for 10 to 15 minutes gives it time to get accustomed to the new vascular flow pattern.
The pedicle of the flap has to be twisted to allow the flap to reach the defect. This should be done after tourniquet release because an empty vessel is more likely to get kinked than a vessel with flow.
Step 7
 The flap is then rotated into the defect and loosely anchored to the edges of the defect using 5-0 nylon sutures (Fig. 44-10).
The flap is then rotated into the defect and loosely anchored to the edges of the defect using 5-0 nylon sutures (Fig. 44-10).

Step 7 Pearls
Keeping the proximal interphalangeal (PIP) and MCP joints in extension will decrease the stretch on the pedicle.
When the flap is used to cover lateral or palmar defects, a folded gauze placed between the fingers that is incorporated into the final dressing keeps the web open and prevents compression of the bridge segment.

Postoperative Care and Expected Outcomes
 A volar splint is used for 1 week to keep the fingers and the wrist in extension. Patients are discharged on the first postoperative day and advised to keep the limb elevated. They are started on range-of-motion exercises at 1 week, the sutures are removed at 2 weeks, and patients are then allowed to resume normal activities (Fig. 44-11).
A volar splint is used for 1 week to keep the fingers and the wrist in extension. Patients are discharged on the first postoperative day and advised to keep the limb elevated. They are started on range-of-motion exercises at 1 week, the sutures are removed at 2 weeks, and patients are then allowed to resume normal activities (Fig. 44-11).


[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 44 Dorsal Metacarpal Artery Perforator Flap
See Video 36: Dorsal Metacarpal Artery Perforator Flap
Indications
Examination/Imaging
Clinical Examination
Surgical Anatomy
Vascular basis: The flap is based on the distal cutaneous perforator of the DMA that arises at the level of the metacarpal neck in the second to fourth intermetacarpal spaces. In addition to the DMA, this flap is also nourished by the palmar arterial system through a dorsopalmar anastomosis. This anastomosis is formed by the dorsal perforating branch of the palmar metacarpal artery (arising from the deep palmar arch) and the DMA at the neck of the metacarpal (Fig. 44-2).
Limits of the flap: We limit our flaps between the distal edge of the extensor retinaculum, the metacarpophalangeal (MCP) joint, and the outer borders of the adjoining metacarpals (Fig. 44-3A and B).
Exposures
Flap design: The DMA perforator closest to the defect is marked at the level of the metacarpal neck in the intermetacarpal space. The location of the perforator represents the pivot point of the flap. The distance between the perforator and the proximal edge of the defect represents the bridge segment of the flap. Based on the size of the soft tissue defect, a flap is designed proximal to the perforator at a distance that equals the bridge segment.
Flaps with a dermoadiposal bridge segment can reach the defect by passing the bridge under a skin tunnel or by laying open the intervening skin segment (Fig. 44-4).
[/not-level-membership-for-surgery-category]
