[level-membership-for-gastroenterology-and-hepatology-category]CASE 44
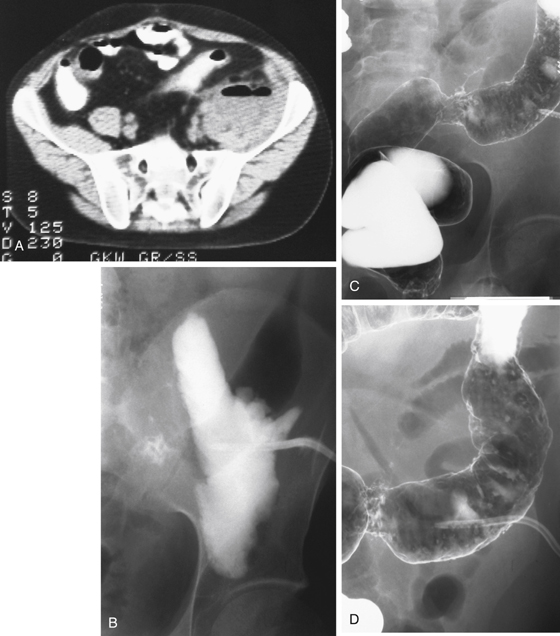
History: A 36-year-old man presents with fever and rigors, left flank and groin pain, and positive psoas sign on examination.
1. Which of the following should be included in the differential for the origin and diagnosis of the disease leading to the imaging finding shown in Figure A? (Choose all that apply.)
C. Crohn’s disease of the small bowel
2. What is the psoas sign?
B. Leg lifting, or flexion of the hip, on the affected side elicits pain.
C. Abdominal pain is elicited by passive flexion and external rotation of the hip.
D. There is dullness to percussion in the left flank.
3. A decision is made to drain the psoas abscess by radiologic intervention. What is the optimal modality to use to undertake this procedure?
4. Worldwide, what is the disease most closely associated with a psoas abscess?
ANSWERS
CASE 44
Psoas Abscess
1. B, C, D, and E
2. B
3. A
4. B
References
Gore RM, Laufer I, Berlin JW. Ulcerative and granulomatous colitis: idiopathic inflammatory bowel disease. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 2nd ed Philadelphia: WB Saunders; 2000:945–992.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, pp 294-297.
Comment
In the modern setting, inflammation in the lower abdomen involving the bowel with extension through to the retroperitoneal psoas muscle has a limited differential diagnosis.
On the right, tuberculosis involving the terminal ileum and cecum is relatively uncommon, except perhaps in AIDS patients, and extension through the retroperitoneum would be unusual. Appendicitis might irritate the psoas, but violation of the retroperitoneum would be uncommon. Thus, the most likely diagnosis in a young patient with an inflammatory phlegmon in the right lower quadrant (RLQ) would be Crohn’s disease with fistulous communication with the retroperitoneum. However, even with Crohn’s disease, a breach of the retroperitoneum is not common.
A differential consideration should include actinomycosis, which, although uncommon, is known to routinely breach fascial and peritoneal barriers. Most of the fistulous communications seen in Crohn’s disease are bowel to bowel, bowel to bladder, bowel to skin, and, on rare occasions, bowel to ureter.
Other conditions in which psoas infiltration can occur are metastatic disease, spinal diseases, and neuromuscular conditions such as neurofibromatosis.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 44
History: A 36-year-old man presents with fever and rigors, left flank and groin pain, and positive psoas sign on examination.
1. Which of the following should be included in the differential for the origin and diagnosis of the disease leading to the imaging finding shown in Figure A? (Choose all that apply.)
C. Crohn’s disease of the small bowel
2. What is the psoas sign?
B. Leg lifting, or flexion of the hip, on the affected side elicits pain.
C. Abdominal pain is elicited by passive flexion and external rotation of the hip.
D. There is dullness to percussion in the left flank.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
