CASE 43
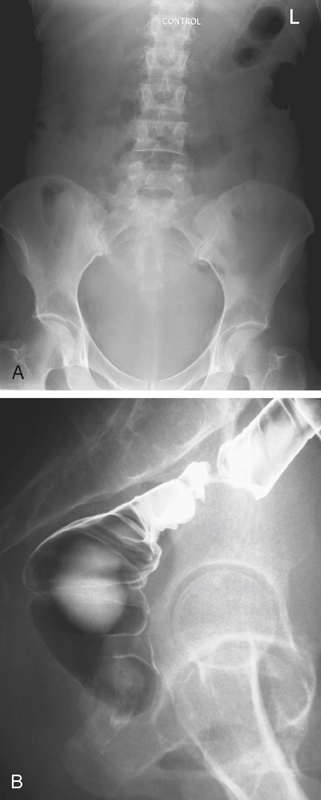
History: A 44-year-old woman presents with 1-year history of constipation and cramping lower abdominal pain.
1. Which of the following should be included in the differential diagnosis of the location and diagnosis in the imaging finding shown in figure A? (Choose all that apply.)
B. Urinary bladder; e.g., outlet obstruction
2. Based on the figures, which of the following is the most likely diagnosis?
B. Urinary bladder outlet obstruction
3. Apart from her colon, what other organ system is most commonly compromised by a pelvic mass?
4. How do malignant and benign pelvic lesions affect the bowel differently?
A. Malignant masses obstruct the bowel, benign lesions do not.
B. Malignant masses ulcerate and fistulate into the adjacent bowel, benign lesions do not.
ANSWERS
CASE 43
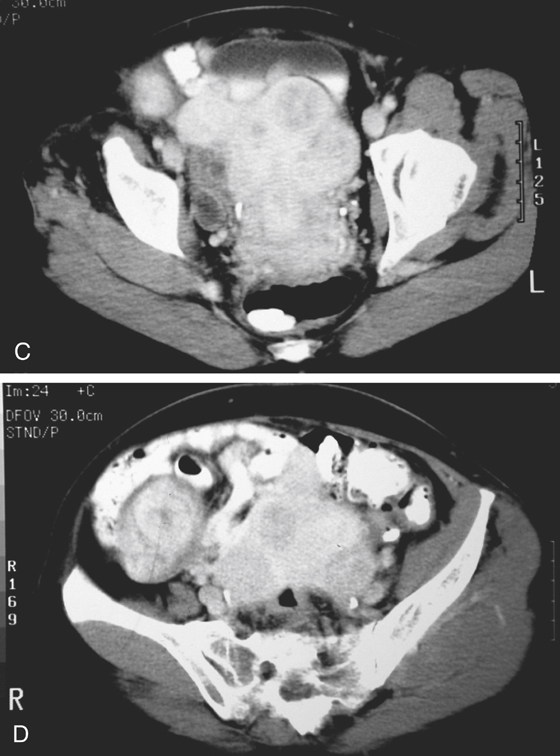
Pelvic Mass Impressing Rectum
1. A, B, D, and E
2. A
3. B
4. D
Reference
Szucs RA, Wolf EL, Gramm HF, et al: Extracolonic diseases involving the colon. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 2nd ed Philadelphia: WB Saunders; 2000:1097–1102.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 291.
Comment
Large masses in the pelvis are quite common in women and are usually related to uterine fibroids. They can vary in size and appearance. Some can be solid, some have necrotic foci within them, and many have calcifications. If the mass is sufficiently large, it can compress the rectum, sigmoid, or descending colon, causing symptoms by its sheer bulk, such as in the images shown with this case. If the mass is malignant, it can invade the bowel from its serosal surface, causing narrowing, irregularity, and tethering of the bowel. Distention of such a segment of bowel is usually exceptionally painful, so keep this in mind when doing barium enemas as part of the workup on patients with possible malignant disease in the pelvis. The other issue (which is best addressed with CT) is the possibility of compression of one or both ureters and hydronephrosis.






