[level-membership-for-surgery-category]
Procedure 42 Cleft Hand Reconstruction




Examination/Imaging
Clinical Examination
 A cleft hand is considered a longitudinal deficiency affecting the central digits. It is commonly inherited as an autosomal dominant trait with variable penetrance. The condition may be bilateral and may involve the feet. Manske and Halikis have proposed a classification based on the status of the first web space that is useful in planning treatment (Table 42-1).
A cleft hand is considered a longitudinal deficiency affecting the central digits. It is commonly inherited as an autosomal dominant trait with variable penetrance. The condition may be bilateral and may involve the feet. Manske and Halikis have proposed a classification based on the status of the first web space that is useful in planning treatment (Table 42-1).

 There is a strong genetic component associated with hand clefts, and genetic counseling is helpful.
There is a strong genetic component associated with hand clefts, and genetic counseling is helpful.
Table 42-1 Classification of Cleft Hand (Manske and Halikis)
| Type | Description | Characteristics |
|---|---|---|
| I | Normal web | Thumb web space is not narrow |
| IIA | Mildly narrowed web | Thumb web space is mildly narrow |
| IIB | Severely narrowed web | Thumb web space is severely narrowed |
| III | Syndactylized web | Thumb and index rays syndactylized, web space obliterated |
| IV | Merged web | Index ray suppressed, thumb web space merged with the cleft |
| V | Absent web | Thumb elements suppressed, ulnar rays remain, thumb web space no longer present |



Exposures
 In children who have a central cleft with narrow thumb and index finger web, the skin over the dorsum of the cleft is raised as a palmar-based flap. This flap is used to resurface the narrow thumb and index finger web after it is released. Elevating this flap on the dorsum is easier because of a lack of adhering palmar fascia. Additionally, this allows access to the metacarpal heads that can be sutured together to close the cleft.
In children who have a central cleft with narrow thumb and index finger web, the skin over the dorsum of the cleft is raised as a palmar-based flap. This flap is used to resurface the narrow thumb and index finger web after it is released. Elevating this flap on the dorsum is easier because of a lack of adhering palmar fascia. Additionally, this allows access to the metacarpal heads that can be sutured together to close the cleft.

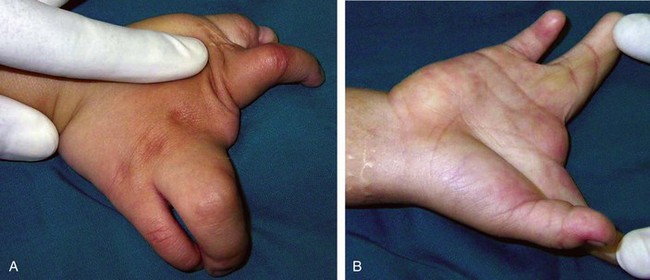
 Figures 42-1 and 42-2 show a 2-year-old boy with a central cleft between the index and long fingers, a tight thumb and index finger web space, and complete complex syndactyly between the long and ring fingers. The syndactyly will need to be released in a second operation.
Figures 42-1 and 42-2 show a 2-year-old boy with a central cleft between the index and long fingers, a tight thumb and index finger web space, and complete complex syndactyly between the long and ring fingers. The syndactyly will need to be released in a second operation.

Procedure
Cleft Hand Reconstruction
Step 1: Elevation of Palmar-Based Cleft Flap
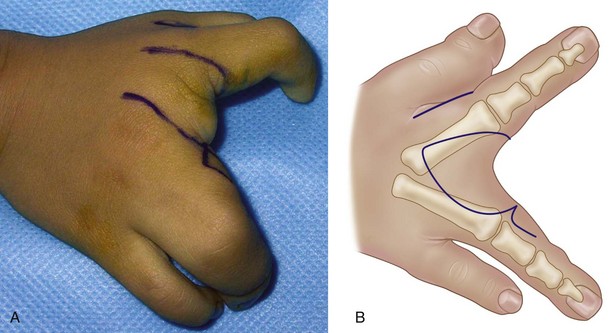
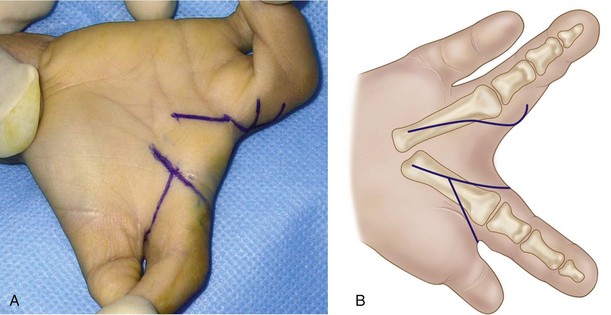
 A palmar-based flap is designed, extending to the dorsum of the hand by parallel incisions (Figs. 42-3 and 42-4).
A palmar-based flap is designed, extending to the dorsum of the hand by parallel incisions (Figs. 42-3 and 42-4).
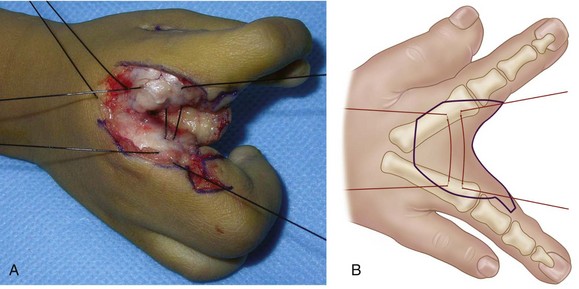
 The parallel incisions are connected on the dorsum, and the dorsal flap is elevated superficial to the extensor tendons (Fig. 42-5).
The parallel incisions are connected on the dorsum, and the dorsal flap is elevated superficial to the extensor tendons (Fig. 42-5).
 The neurovascular bundles are identified on the palmar aspect and protected, and the flap is mobilized by dividing any strands of palmar fascia (Fig. 42-6).
The neurovascular bundles are identified on the palmar aspect and protected, and the flap is mobilized by dividing any strands of palmar fascia (Fig. 42-6).


Step 2: Release of Thumb and Index Finger Web Space


Step 3: Closure of Cleft




Step 4: Transfer of Cleft Flap to Resurface Thumb and Index Finger Web


Step 5: Creation of New Web Space in Cleft







Postoperative Care and Expected Outcomes


[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 42 Cleft Hand Reconstruction
Examination/Imaging
Clinical Examination
A cleft hand is considered a longitudinal deficiency affecting the central digits. It is commonly inherited as an autosomal dominant trait with variable penetrance. The condition may be bilateral and may involve the feet. Manske and Halikis have proposed a classification based on the status of the first web space that is useful in planning treatment (Table 42-1).
There is a strong genetic component associated with hand clefts, and genetic counseling is helpful.
Table 42-1 Classification of Cleft Hand (Manske and Halikis)
| Type | Description | Characteristics |
|---|---|---|
| I | Normal web | Thumb web space is not narrow |
| IIA | Mildly narrowed web | Thumb web space is mildly narrow |
| IIB | Severely narrowed web | Thumb web space is severely narrowed |
| III | Syndactylized web | Thumb and index rays syndactylized, web space obliterated |
| IV | Merged web | Index ray suppressed, thumb web space merged with the cleft |
| V | Absent web | Thumb elements suppressed, ulnar rays remain, thumb web space no longer present |
