Procedure 41 Centralization for Radial Longitudinal Deficiency
 See Video 34: Centralization for Radial Deficiency
See Video 34: Centralization for Radial Deficiency
Indications
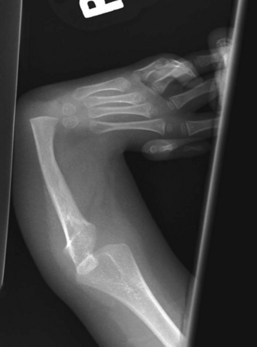
 Radial longitudinal deficiency (RLD) has been classified into four grades depending on the degree of hypoplasia of the radius (Table 41-1). Centralization is usually performed at 9 to 12 months of age because anesthesia is safer, preliminary soft tissue distraction can be carried out, and subsequent thumb reconstruction can be done before the child develops a maladaptive pattern.
Radial longitudinal deficiency (RLD) has been classified into four grades depending on the degree of hypoplasia of the radius (Table 41-1). Centralization is usually performed at 9 to 12 months of age because anesthesia is safer, preliminary soft tissue distraction can be carried out, and subsequent thumb reconstruction can be done before the child develops a maladaptive pattern.
 This procedure may be done first for children with type 0 or 1 deficiencies.
This procedure may be done first for children with type 0 or 1 deficiencies.

| Type | Distal Radius | Proximal Radius |
|---|---|---|
| N | Normal | Normal |
| 0 | Normal | Normal, radioulnar synostosis, congenital radial head dislocation |
| 1 | >2 mm shorter than ulna | Normal, radioulnar synostosis, congenital radial head dislocation |
| 2 | Hypoplasia | Hypoplasia |
| 3 | Physis absent | Variable hypoplasia |
| 4 | Absent | Absent |
Examination/Imaging
Clinical Examination
 Sixty percent to 70% of children with RLD have an associated systemic or musculoskeletal abnormality, the most common being scoliosis. Therefore, before surgery, all children with RLD should undergo a thorough musculoskeletal and systemic examination, including spinal radiographs, cardiac echocardiographic evaluation, renal ultrasound, and a complete blood count.
Sixty percent to 70% of children with RLD have an associated systemic or musculoskeletal abnormality, the most common being scoliosis. Therefore, before surgery, all children with RLD should undergo a thorough musculoskeletal and systemic examination, including spinal radiographs, cardiac echocardiographic evaluation, renal ultrasound, and a complete blood count.


Surgical Anatomy






Exposures
 The four key steps of centralization are the following:
The four key steps of centralization are the following:
Procedure
Step 1: Preliminary Soft Tissue Distraction
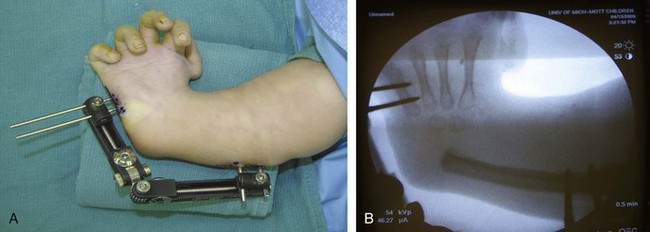
 A uniplanar external fixator device is applied on the ulnar side of the affected limb (the metacarpal of small finger and ulna of patient shown in Figure 41-4). This is best done at 6 to 9 months of age.
A uniplanar external fixator device is applied on the ulnar side of the affected limb (the metacarpal of small finger and ulna of patient shown in Figure 41-4). This is best done at 6 to 9 months of age.

 Distraction is continued until the hand is about in a neutral position. Normally, it takes about 2 months of distraction to achieve this position (Fig. 41-5).
Distraction is continued until the hand is about in a neutral position. Normally, it takes about 2 months of distraction to achieve this position (Fig. 41-5).
 The external fixator device can be removed at the same time as surgery for centralization.
The external fixator device can be removed at the same time as surgery for centralization.

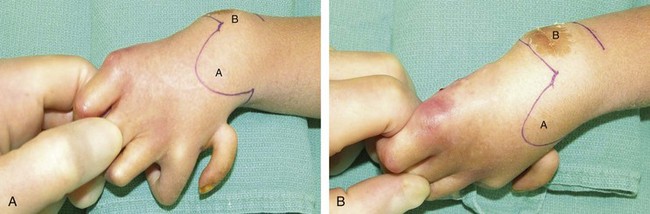
Step 2: Elevation of Bilobed Flap
 The skin is incised along the previously marked bilobed flap.
The skin is incised along the previously marked bilobed flap.
 The flap is raised in a plane superficial to the extensor retinaculum.
The flap is raised in a plane superficial to the extensor retinaculum.
Step 2 Pitfalls
Care should be taken to preserve the superficial cutaneous nerves and longitudinal veins.
Flaps should be kept as thick as possible to avoid devascularizing the wound edges.
Beware of the large dorsal branch of the median nerve, which replaces the absent superficial radial nerve that supplies sensation to the radial aspect of the hand. This branch is positioned in the subcutaneous fold between the wrist and forearm.
Step 3: Dissection of Nerve and Tendons
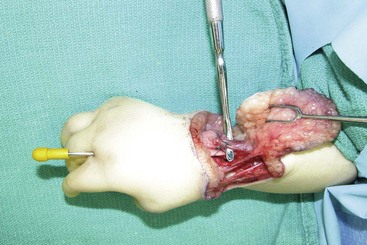
 The median nerve must be identified first during the exposure. It is the most superficial structure on the radial side of the distal forearm and can easily be confused with a tendinous structure (Fig. 41-6).
The median nerve must be identified first during the exposure. It is the most superficial structure on the radial side of the distal forearm and can easily be confused with a tendinous structure (Fig. 41-6).
 The extensor carpi ulnaris (ECU) is easier to find distal to the retinaculum. The ECU is shortened by imbrication after centralization, and the ECR is divided at its insertion to facilitate later transfer to the ECU (Fig. 41-7).
The extensor carpi ulnaris (ECU) is easier to find distal to the retinaculum. The ECU is shortened by imbrication after centralization, and the ECR is divided at its insertion to facilitate later transfer to the ECU (Fig. 41-7).



Step 4: Ulnocarpal Joint Reduction and Centralization
 The wrist capsule is opened distal to the ulnar physis, and a soft tissue release is carried out until the carpus can be brought over the distal ulna (Fig. 41-8).
The wrist capsule is opened distal to the ulnar physis, and a soft tissue release is carried out until the carpus can be brought over the distal ulna (Fig. 41-8).


Step 4 Pearls
If the carpus cannot be reduced, the radial side of the wrist needs to be reexamined, and any radial fibrous bands should be divided to facilitate reduction of the carpus onto the ulna.
Occasionally, partial carpectomy or limited shaving of the carpus to create a notch in it for seating of the distal end of the ulna may be required to achieve reduction. However, it should be remembered that carpal bones are resected only if reduction is impossible, because excessive resection of the epiphysis will arrest growth. Rather than accepting this risk, preoperative soft tissue stretching using an external distractor is recommended in most cases.
Step 5: Fixation


Step 6: Wrist Stabilization
 The ECR tendon is transferred to the distal stump of the ECU passing below the EDC (see Fig. 41-3). The proximal end of the ECU is advanced and sutured to the dorsal wrist capsule. Tendon repairs are done using 2-0 Ethibond horizontal mattress sutures.
The ECR tendon is transferred to the distal stump of the ECU passing below the EDC (see Fig. 41-3). The proximal end of the ECU is advanced and sutured to the dorsal wrist capsule. Tendon repairs are done using 2-0 Ethibond horizontal mattress sutures.
 The extensor retinaculum is repaired using 4-0 Vicryl, and skin is closed with 4-0 chromic sutures (Fig. 41-10).
The extensor retinaculum is repaired using 4-0 Vicryl, and skin is closed with 4-0 chromic sutures (Fig. 41-10).

Postoperative Care and Expected Outcomes
 A long-arm cast with the elbow flexed to 90 degrees is provided. The extremity is immobilized for at least 8 weeks, and the pin is kept in place for as long as possible. A long-arm Orthoplast splint to maintain wrist position is worn full-time for 3 months and then at night until skeletal maturity. Prolonged pin fixation followed by long-term splinting is necessary to minimize recurrence.
A long-arm cast with the elbow flexed to 90 degrees is provided. The extremity is immobilized for at least 8 weeks, and the pin is kept in place for as long as possible. A long-arm Orthoplast splint to maintain wrist position is worn full-time for 3 months and then at night until skeletal maturity. Prolonged pin fixation followed by long-term splinting is necessary to minimize recurrence.



