[level-membership-for-cardiovascular-category]
CASE 41

History: A patient presents with fatigue.
1. Which cardiac chambers are enlarged? (Choose all that apply.)
A. Left atrium
C. Right atrium
2. What is the most likely diagnosis?
3. What is the most common cause of mitral stenosis?
A. Trauma
B. Congenital
4. Which of the following lesions most commonly mimics the symptoms of mitral stenosis?
A. Lipoma
B. Myxoma
C. Rhabdomyoma
D. Fibroma
ANSWERS
References
Bonow RO, Cheitlin MD, Crawford MH, et al. Task Force 3: valvular heart disease. J Am Coll Cardiol. 2005;45(8):1334–1340.
Walker CM, Reddy GP, Steiner RM. Radiology of the heart. In: Rosendorff C, ed. Essential Cardiology. ed 3 Philadelphia: Saunders; 2012.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 186–191.
Comment
Etiology
Mitral stenosis is usually acquired and develops approximately 5 to 10 years after an episode of rheumatic heart disease. Other causes of left atrial enlargement include prolapse of a left atrial myxoma or thrombus, amyloid, and carcinoid syndrome.
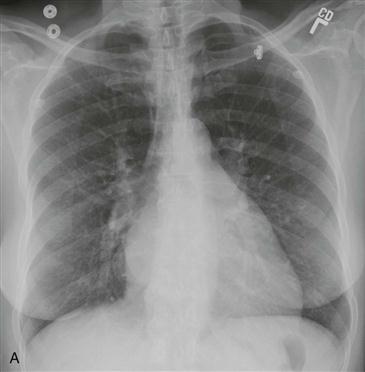
Radiography
Chest radiographs demonstrate the effects of pulmonary venous hypertension. The left atrium is enlarged, and the left ventricle is normal in size (Figs. A and B). Disproportionate enlargement of the left atrial appendage is often seen in rheumatic mitral stenosis. The mitral valve may contain nodular, amorphous calcification. Pulmonary interstitial edema is a frequent finding. Uncommonly, patients develop hemosiderosis and ossification of pulmonary nodules.
Cross-Sectional Imaging
Further evaluation involves echocardiography. The area of the valve is measured, and valve mobility, thickening of the leaflets, and submitral scarring are assessed. Velocity-encoded cine phase contrast MRI can be performed to quantify the severity of stenosis. The pressure gradient across the valve can be calculated by use of the modified Bernoulli equation, ΔP = 4v2, where P is the pressure in mm Hg and v is peak velocity in m/sec. The peak velocity can be estimated by echocardiography or by velocity-encoded cine phase contrast MRI.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
CASE 41
History: A patient presents with fatigue.
1. Which cardiac chambers are enlarged? (Choose all that apply.)
A. Left atrium
C. Right atrium
2. What is the most likely diagnosis?
3. What is the most common cause of mitral stenosis?
A. Trauma
B. Congenital
[/not-level-membership-for-cardiovascular-category]
