[level-membership-for-anesthesiology-category]
CHAPTER 40 Chronic Obstructive Pulmonary Disease






3 Describe chronic bronchitis and emphysema
 Chronic bronchitis: Characterized by cough, sputum production, recurrent infection, and airway obstruction for many months to several years. Patients with chronic bronchitis have mucous gland hyperplasia, mucus plugging, inflammation and edema, peribronchiolar fibrosis, airway narrowing, and bronchoconstriction. Decreased airway lumina caused by mucus and inflammation increase resistance to flow of gases.
Chronic bronchitis: Characterized by cough, sputum production, recurrent infection, and airway obstruction for many months to several years. Patients with chronic bronchitis have mucous gland hyperplasia, mucus plugging, inflammation and edema, peribronchiolar fibrosis, airway narrowing, and bronchoconstriction. Decreased airway lumina caused by mucus and inflammation increase resistance to flow of gases.
4 List contributory factors associated with the development of chronic obstructive pulmonary disease
 Smoking: Smoking impairs ciliary function, depresses alveolar macrophages; leads to increased mucous gland proliferation and mucus production; increases the inflammatory response in the lung; leading to increased proteolytic enzyme release; reduces surfactant integrity; and causes increased airway reactivity.
Smoking: Smoking impairs ciliary function, depresses alveolar macrophages; leads to increased mucous gland proliferation and mucus production; increases the inflammatory response in the lung; leading to increased proteolytic enzyme release; reduces surfactant integrity; and causes increased airway reactivity.









6 What features distinguish pink puffers from blue bloaters?
| Pink puffers (emphysema) | Blue bloaters (chronic bronchitis) |
| Usually older (>60 years) | Relatively young |
| Pink in color | Cyanotic |
| Thin | Heavier in weight |
| Minimal cough | Chronic productive cough; frequent wheeze |










9 How does a chronically elevated arterial carbon dioxide partial pressure affect the respiratory drive in a person with chronic obstructive pulmonary disease?
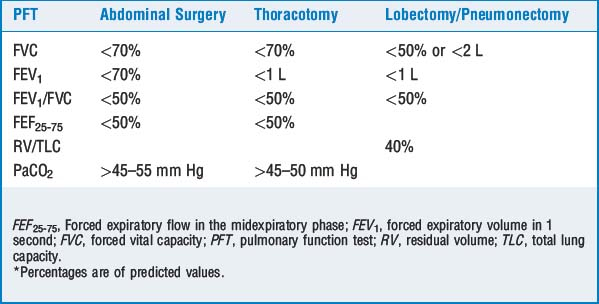
12 What factors are associated with an increased perioperative morbidity or mortality?
Patients presenting for lobectomy or pneumonectomy must have pulmonary function and arterial blood gas values that are superior to the values in Table 40-1. If any of the aforementioned criteria are not satisfied, further preoperative testing is indicated to determine the risk-benefit ratio for lung resection. Further tests include split-lung function, regional perfusion, regional ventilation, regional bronchial balloon occlusion, and pulmonary artery balloon occlusion studies. A forced expiratory volume in 1 second (FEV1) less than 800 ml in a 70-kg person is probably incompatible with life and is an absolute contraindication to lung resection because of the high incidence for extended mechanical ventilation.
13 List the common pharmacologic agents used to treat COPD and their mechanisms of action
TABLE 40-2 Agents used to Treat Chronic Obstructive Pulmonary Disease
| Class and Examples | Actions |
|---|---|
| β-Adrenergic agonists: albuterol, metaproterenol, fenoterol, terbutaline, epinephrine | Increases adenylate cyclase, increasing cAMP and decreasing smooth muscle tone (bronchodilation); short-acting β-adrenergic agonists (e.g., albuterol, terbutaline, and epinephrine) are the agents of choice for acute exacerbations |
| Methylxanthines: aminophylline, theophylline | Phosphodiesterase inhibition increases cAMP; potentiates endogenous catecholamines; improves diaphragmatic contractility; central respiratory stimulant |
| Corticosteroids: methylprednisolone, dexamethasone, prednisone, cortisol | Antiinflammatory and membrane stabilizing; inhibits histamine release; potentiates β-agonists |
| Anticholinergics: atropine, glycopyrrolate, ipratropium | Blocks acetylcholine at postganglionic receptors, decreasing cGMP, relaxing airway smooth muscle |
| Cromolyn sodium | Also a membrane stabilizer, preventing mast cell degranulation, but must be given prophylactically |
| Antileukotrienes: zileuton, montelukast | Inhibition of leukotriene production and/or zafirlukast, leukotriene antagonism; antiinflammatory; used in addition to corticosteroids; however, may be considered first-line antiinflammatory therapy for patients who cannot or will not use corticosteroids |
cAMP, Cyclic adenosine monophosphate; cGMP, cyclic guanosine monophosphate.
14 What therapies are available to reduce perioperative pulmonary risk?








15 Do advantages exist with regional anesthesia techniques in patients with chronic obstructive pulmonary disease?
17 Discuss the particular concerns regarding muscle relaxation (and reversal) in patients with chronic obstructive pulmonary disease
19 Define auto-PEEP
KEY POINTS: Chronic Obstructive Pulmonary Disease 








21 How would you treat intraoperative bronchospasm?
 Administer 100% oxygen and manually ventilate, allowing sufficient expiratory time. Identify and correct the underlying condition as discussed in Question 20.
Administer 100% oxygen and manually ventilate, allowing sufficient expiratory time. Identify and correct the underlying condition as discussed in Question 20.






23 Should H2-receptor antagonists be avoided in patients with chronic obstructive pulmonary disease?
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 40 Chronic Obstructive Pulmonary Disease
3 Describe chronic bronchitis and emphysema
Chronic bronchitis: Characterized by cough, sputum production, recurrent infection, and airway obstruction for many months to several years. Patients with chronic bronchitis have mucous gland hyperplasia, mucus plugging, inflammation and edema, peribronchiolar fibrosis, airway narrowing, and bronchoconstriction. Decreased airway lumina caused by mucus and inflammation increase resistance to flow of gases.4 List contributory factors associated with the development of chronic obstructive pulmonary disease
Smoking: Smoking impairs ciliary function, depresses alveolar macrophages; leads to increased mucous gland proliferation and mucus production; increases the inflammatory response in the lung; leading to increased proteolytic enzyme release; reduces surfactant integrity; and causes increased airway reactivity.6 What features distinguish pink puffers from blue bloaters?
| Pink puffers (emphysema) | Blue bloaters (chronic bronchitis) |
| Usually older (>60 years) | Relatively young |
| Pink in color | Cyanotic |
| Thin | Heavier in weight |
| Minimal cough | Chronic productive cough; frequent wheeze |
