[level-membership-for-gastroenterology-and-hepatology-category]CASE 40

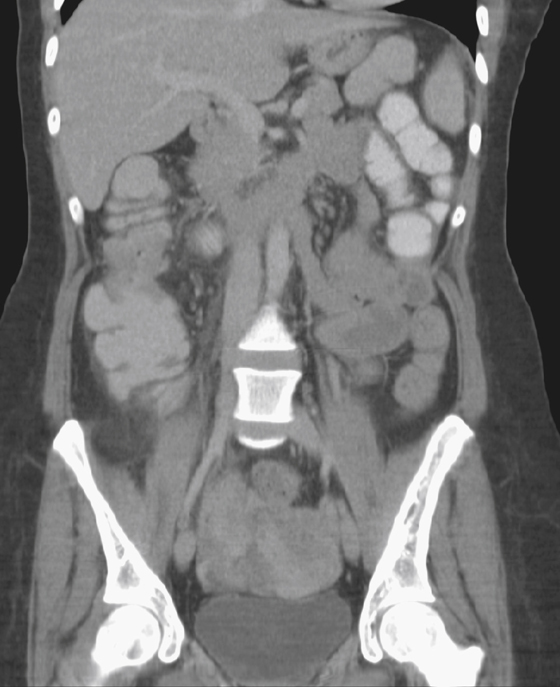


History: A 60-year-old woman presents with blood in her stools.
1. Which of the following should be included in the differential diagnosis of the imaging findings shown? (Choose all that apply.)
2. Several known and accepted risk factors are associated with colorectal cancer. Which of the following is not a risk factor?
3. What is the most common etiology for colorectal carcinoma?
4. Which of the following correctly describes the apple core lesion?
D. The central channel cored out of an obstructive tumor, restoring patency to a hollow viscus
ANSWERS
CASE 40
Colonic Annular Carcinoma
1. A, B, C, and D
2. B
3. A
4. A
References
Dahnert W. Radiology Review Manual. 6th ed Philadelphia: Lippincott Williams & Wilkins; 2007. pp 813-815
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 272.
Comment
Although the incidence of colorectal carcinoma (CRC) has leveled off in the United States in recent years, it is still the fourth most common cancer after prostate, breast, and lung. Its mortality rate is exceeded only by lung cancer at this time. Survival depends on early detection, which in CRC means finding and removing polyps. In polyps between 5 mm and 10 mm there is about a 1% chance of malignancy. In polyps between 1 and 2 cm there is about a 10% risk. As the size of sessile polyps increases, the cancer risk increases; polyps larger than 2 cm have about a 40% risk. Diminutive polyps (less than 5 mm) have little or no risk of malignancy, and the search for diminutive polyps is probably a waste of time, expense, and effort. However, the screening for 1 cm or larger polyps is warranted. This can be done with colonoscopy, which has the added benefit of polyp removal at the time of discovery. However, the complication rate (perforation) is at least 10 times that of the air contrast barium enema (ACBE) and the cost is considerably higher than ACBE. If done by skilled radiologists, the detection rate of polyps 1 cm and larger, as well as CRC, approaches that of colonoscopy. Multidetector computed tomography (MDCT) is now especially useful in detection by evaluation for local, nodal and distant spread (figures 1 to 3). As the number of sites using CT colonoscopy increases, this holds promise as being an excellent screening method in the general population with minimal examination time, no sedation, and rapid results.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 40
History: A 60-year-old woman presents with blood in her stools.
1. Which of the following should be included in the differential diagnosis of the imaging findings shown? (Choose all that apply.)
2. Several known and accepted risk factors are associated with colorectal cancer. Which of the following is not a risk factor?
3. What is the most common etiology for colorectal carcinoma?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
