Procedure 4 Drainage of Purulent Flexor Tenosynovitis
Indications


Examination/Imaging
Clinical Examination
 Purulent flexor tenosynovitis is a clinical diagnosis.
Purulent flexor tenosynovitis is a clinical diagnosis.
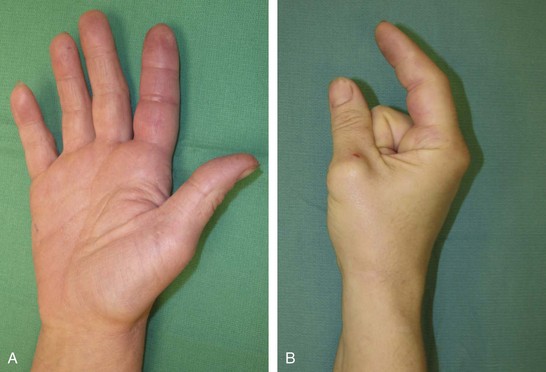
 Kanavel signs (Fig. 4-1A and B) are as follows:
Kanavel signs (Fig. 4-1A and B) are as follows:


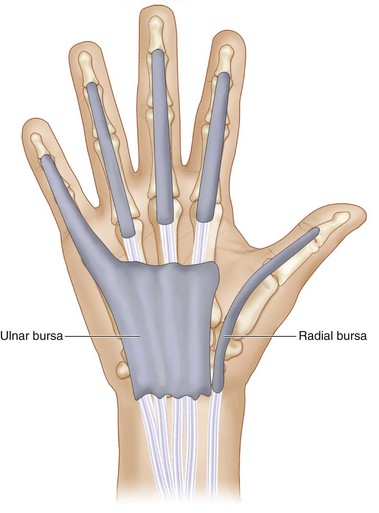
 Tenosynovitis of the thumb and small finger may be less impressive owing to continuity of the fibrous flexor sheath with larger radial and ulnar bursa that allow spontaneous decompression (Fig. 4-2).
Tenosynovitis of the thumb and small finger may be less impressive owing to continuity of the fibrous flexor sheath with larger radial and ulnar bursa that allow spontaneous decompression (Fig. 4-2).
 Infection of the thumb may spread to the small finger and vice versa.
Infection of the thumb may spread to the small finger and vice versa.
 Examine for signs of gout or other intra-articular processes, which are treated medically.
Examine for signs of gout or other intra-articular processes, which are treated medically.
 Examine for symptoms not confined to one joint. (Gout is typically monoarticular.)
Examine for symptoms not confined to one joint. (Gout is typically monoarticular.)


Surgical Anatomy








Exposures
 Distal exposure is though a longitudinal midaxial incision dorsal to the Cleland ligament, just proximal to the DIP joint on the side opposite the pinch surface, except for the small finger, where the incision is placed radially to avoid the resting ulnar side of the small finger (Fig. 4-3).
Distal exposure is though a longitudinal midaxial incision dorsal to the Cleland ligament, just proximal to the DIP joint on the side opposite the pinch surface, except for the small finger, where the incision is placed radially to avoid the resting ulnar side of the small finger (Fig. 4-3).



Pearls
Plan all incisions so that they may be extended distally or proximally as necessary.
Wide exposure of the entire fibrous flexor sheath is reserved for failure of limited exposure. The need for wide exposure is rare and can be associated with exposure of the tendon sheath and neurovascular structures, which leads to desiccation. Most early infections can be treated effectively with antibiotics, hand splinting in intrinsic plus position, and elevation. If the infection does not improve—based on the extent of the erythema and decreased pain—surgical drainage is necessary by the irrigation technique described in this chapter.
Extending the palmar incision proximally may be necessary if the infection has breached the fibrous flexor sheath.
In rare circumstances with ascending infection, a carpal tunnel exposure or volar forearm exposure may be necessary.
Procedure
Step 1: Distal Exposure of the Fibrous Flexor Sheath
 Any contaminated puncture wounds should be thoroughly débrided and irrigated.
Any contaminated puncture wounds should be thoroughly débrided and irrigated.
 A 1-cm midaxial longitudinal incision is made dorsal to the Cleland ligament on the noncontact surface of the finger overlying the A5 pulley (see Fig. 4-3).
A 1-cm midaxial longitudinal incision is made dorsal to the Cleland ligament on the noncontact surface of the finger overlying the A5 pulley (see Fig. 4-3).

 The sheath is entered by sharply dividing the A5 pulley longitudinally over a distance of 5 mm.
The sheath is entered by sharply dividing the A5 pulley longitudinally over a distance of 5 mm.

Step 1 Pearls
In tenosynovitis, in which an atypical infection is expected, it is important to send the appropriate specimens: Gram stain, culture, sensitivity, acid-fast bacillus stain and culture, nontuberculous mycobacteria culture, fungus stain, and mycotic culture.
If a puncture wound is identified, it is advisable to include this wound in the exposure.
Step 2: Proximal Exposure of Fibrous Flexor Sheath




Step 3: Closed Tendon Sheath Irrigation
 A 16-gauge intravenous catheter is introduced proximally into the fibrous flexor sheath under the A1 pulley (see Fig. 4-4).
A 16-gauge intravenous catheter is introduced proximally into the fibrous flexor sheath under the A1 pulley (see Fig. 4-4).


 Drainage wicks should be placed in the proximal and distal incisions, which are left open.
Drainage wicks should be placed in the proximal and distal incisions, which are left open.
 Continuous irrigation is not used.
Continuous irrigation is not used.
 The tourniquet is released, hemostasis is achieved, and the incisions are closed loosely.
The tourniquet is released, hemostasis is achieved, and the incisions are closed loosely.
Step 3 Pearls
An irrigation catheter may be secured in place for continuous or periodic irrigation after the operation, if there is concern about more contamination in the tendon sheath. The need for irrigation of the tendon sheath on the ward is infrequent. It is preferable to irrigate gently through the catheter every 8 hours for 24 hours.
Step 3 Pitfalls
High-pressure irrigation may spread the infection.
One must be careful not to flush the irrigant into the subcutaneous tissue because this will cause marked swelling in the finger, resulting in finger compartment syndrome.
The fluid should flow readily through the tendon sheath until clear effluent is seen in the distal incision.
Postoperative Care and Expected Outcomes
 The arm and fingers should be immobilized in a bulky splint and elevated.
The arm and fingers should be immobilized in a bulky splint and elevated.


 Adequate analgesia is necessary to begin early motion.
Adequate analgesia is necessary to begin early motion.
 The incisions typically heal without specific treatment, but edema may persist for weeks.
The incisions typically heal without specific treatment, but edema may persist for weeks.

 Ten to 20% of patients fail to recover full motion.
Ten to 20% of patients fail to recover full motion.
 About 66% of motion is achieved by 6 weeks, improving to 80% by 30 months.
About 66% of motion is achieved by 6 weeks, improving to 80% by 30 months.
Abrams RA, Botte MJ. Hand infections: treatment recommendations for specific types. J Am Acad Orthop Surg. 1996;4:219-230.
Lille S, Hayakawa T, Neumeister MW, et al. Continuous postoperative catheter irrigation is not necessary for the treatment of suppurative flexor tenosynovitis. J Hand Surg [Br]. 2000;25:304-307.
Neviaser RJ. Closed tendon sheath irrigation for pyogenic flexor tenosynovitis. J Hand Surg [Am]. 1978;3:462-466.
Pang HN, Teoh LC, Yam AKT, et al. Factors affecting the prognosis of pyogenic flexor tenosynovitis. J Bone Joint Surg [Am]. 2007;89:1742-1748.


