CASE 4 Coronary Aneurysm
Cardiac catheterization
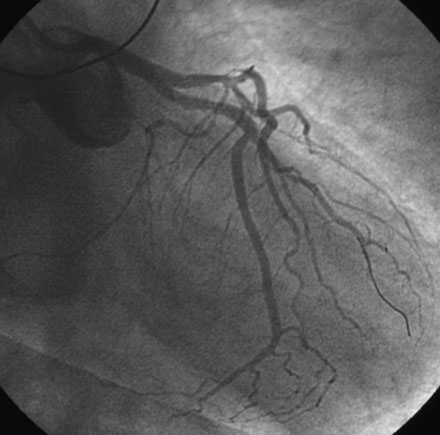
Ventriculography revealed normal left ventricular function. The left coronary artery was angiographically normal. Right coronary angiography, however, demonstrated a large focal aneurysm of the proximal coronary artery, measuring nearly 10 mm in diameter, with a moderate stenosis in the midsegment of the vessel (Figure 4-1 and Videos 4-1, 4-2).

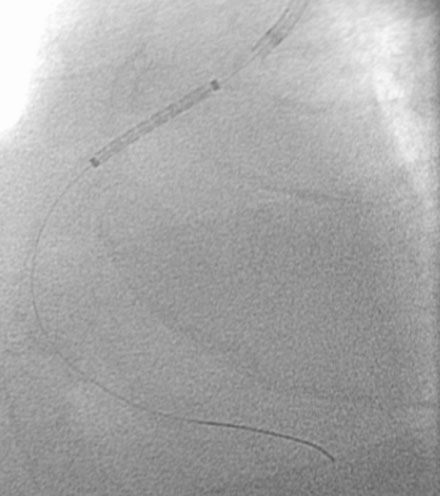
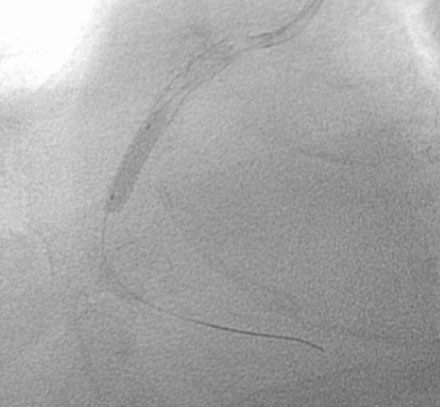
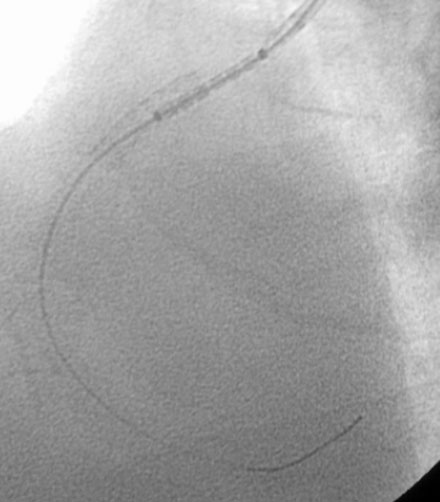
Following the diagnostic cardiac catheterization, the various treatment options were discussed in detail, including medical therapy, surgery, and percutaneous treatment using a covered stent. After much discussion, the patient chose to undergo treatment with a covered stent. After loading with 300 mg of clopidogrel, the patient returned to the cardiac catheterization laboratory for this procedure. Bivalirudin was used as the procedural anticoagulant. The operator engaged the right coronary artery with an 8 French right Judkins guide and positioned an extra-support 0.014” guidewire distally. A 5.0 mm diameter, 22 mm long polytetrafluoroethylene (PTFE) covered stent (Atrium iCast, Atrium Medical Corporation) was centered over the aneurysm (Figure 4-2) and deployed. The angiogram obtained after stent deployment showed a small residual leak into the aneurysm sac at the proximal end of the stent (Figure 4-3 and Video 4-3). The operator proceeded with placement of a 4.0 mm diameter by 15 mm long bare-metal stent at the moderate stenosis in the midsegment of the vessel (Figure 4-4), resulting in an excellent angiographic result at this site; however, there remained a small leak into the aneurysm (Video 4-4). A second covered stent (5.0 mm diameter by 16 mm long) was used to cover this small residual leak (Figure 4-5). This resulted in complete exclusion of the aneurysm from the coronary circulation (Figure 4-6 and Videos 4-5, 4-6).


Discussion
Coronary aneurysms represent abnormal dilatation of the coronary artery and are typically defined by the presence of an enlarged segment greater than 1.5 times the diameter of a normal adjacent segment.1–3 Coronary aneurysms are not common. They are observed in between 1.5% and 5% of patients undergoing coronary angiography.1 Similar to this case, they more commonly affect the right coronary artery; the left anterior descending artery is next most commonly involved, followed by the circumflex artery. Multiple aneurysms are frequently observed, but aneurysms of the left main stem are very rare.
By far, the most common cause is atherosclerotic degeneration, accounting for at least 50% of aneurysms. Kawasaki disease is the most common cause worldwide and is the most common nonatherosclerotic cause. Other etiologies are rare and include infection, polyarteritis nodosa, Takayasu arteritis, and connective tissue disorders (Marfan and Ehlers-Danlos syndromes). Coronary aneurysms may also arise iatrogenically from deep vessel injury induced by balloon angioplasty, coronary stenting, or coronary atherectomy procedures. Recently, they have been observed after drug-eluting stent placement.4
Many coronary aneurysms are asymptomatic and found incidentally on coronary angiography; however, they may be responsible for symptoms including angina and myocardial infarction. Myocardial infarction can arise from distal embolization or from in-situ thrombosis.5 Fortunately, rupture of a coronary artery aneurysm is an exceedingly rare occurrence and is only a concern when there is massive enlargement.
There is no consensus regarding the optimal therapy for coronary aneurysms. Most physicians base their therapeutic decision on the size of the aneurysm, the presence of coexisting obstructive lesions, and evidence of ischemia or infarction. Medical therapy with antiplatelet agents and possibly warfarin might reduce the chance of embolization or thrombosis. Surgery is reserved for very large aneurysms involving multiple segments or extending over a long segment. As demonstrated in this case, covered stents are effective at excluding the aneurysm from the coronary circulation but their large bulky nature may result in technical difficulties with delivery.6 They are also not specifically approved for this indication.
1 Chrissoheris M.P., Donohue T.J., Young R.S.K., Ghantous A. Coronary artery aneurysms. Cardiol Rev. 2008;16:116-123.
2 Syed M., Lesch M. Coronary artery aneurysm: A review. Prog Cardiovasc Dis. 1997;40:77-84.
3 Robinson F.C. Aneurysms of the coronary arteries. Am Heart J. 1985;109:129-135.
4 Aoki J., Kirtane A., Leon M.B., Dangas G. Coronary artery aneurysms after drug-eluting stent implantation. JACC Cardiovasc Interv. 2008;1:14-21.
5 von Rotz F., Niederhauser U., Straumann E., Kurz D., Bertel O., Turina M.I. Myocardial infarction caused by a large coronary artery aneurysm. Ann Thorac Surg. 2000;69:1568-1569.
6 Szalat A., Durst R., Cohen A., Lotan C. Use of polytetrafluoroethylene-covered stent for treatment of coronary artery aneurysm. Catheter Cardiovasc Interv. 2005;66:203-208.