CASE 4

History: A patient presents with chest pain.
1. What should be included in the differential diagnosis for air adjacent to the heart seen on the chest radiograph? (Choose all that apply.)
B. Pneumothorax
2. What is the most common cause of this entity?
B. Tumor
C. Infection
3. What would be the best next step in management if this patient were hypotensive and bradycardic?
A. High-flow oxygen (10 L/min)
D. Emergent pericardiocentesis
4. What is the likely mechanism by which barotrauma causes this condition?
A. Pneumothorax
B. Air dissects along the pulmonary vessels
C. Low pressure
ANSWERS
Reference
Katabathina VS, Restrepo CS, Martinez-Jimenez S, et al. Nonvascular, nontraumatic mediastinal emergencies in adults: a comprehensive review of imaging findings. Radiographics. 2011;31(4):1141–1160.
Comment
Imaging
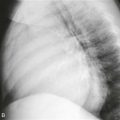
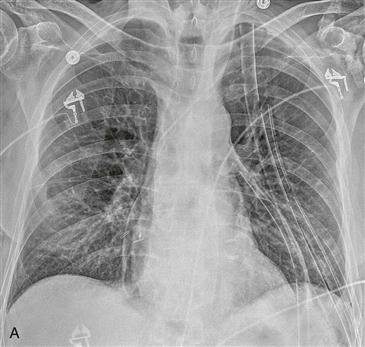
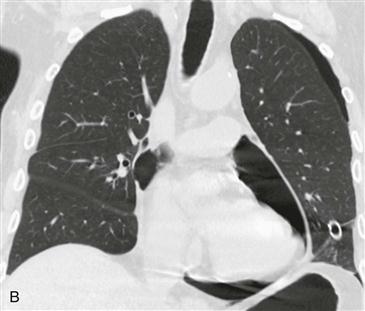
This patient has a large air collection within the pericardial space (Figs. A–C). There is no extension above the level of the pericardial recesses helping to differentiate it from pneumomediastinum (Figs. A and B). This patient did not have clinical signs or symptoms of cardiac tamponade, and serial imaging (not shown) showed resolution of air.
Diagnosis
Pneumopericardium is most commonly caused by trauma. Nontraumatic causes include infective pericarditis with a gas-forming organism, fistulous communication with the gastrointestinal tract or lung, and extension of pneumomediastinum into the pericardial space. Tension pneumopericardium is a life-threatening condition diagnosed in the setting of hemodynamic collapse. Imaging findings on CT or MRI that suggest tamponade physiology include compression of the anterior aspect of the heart, dilated inferior vena cava, and compression or displacement of cardiac chambers. Immediate pericardial decompression is required in patients with cardiac tamponade to prevent death.