Automated External Defibrillation
PREREQUISITE NURSING KNOWLEDGE
• Defibrillation is the therapeutic use of an electrical shock that temporarily stops or stuns an irregularly beating heart and allows the spontaneously repolarizing pacemaking cells within the heart to recover and resume more normal electrical activity. Ventricular fibrillation (VF) and ventricular tachycardia (VT) are the only two rhythms recognized as shockable by an automated external defibrillator (AED) (Fig. 39-1).

• Time is the major determining factor in the success rates of defibrillation. For every minute defibrillation is delayed, the chance of success decreases by 7% to 10%.1,2,5 When used in conjunction with effective CPR, the decrease in the likelihood of success is more gradual and averages 3% to 4% per minute.1,2,5
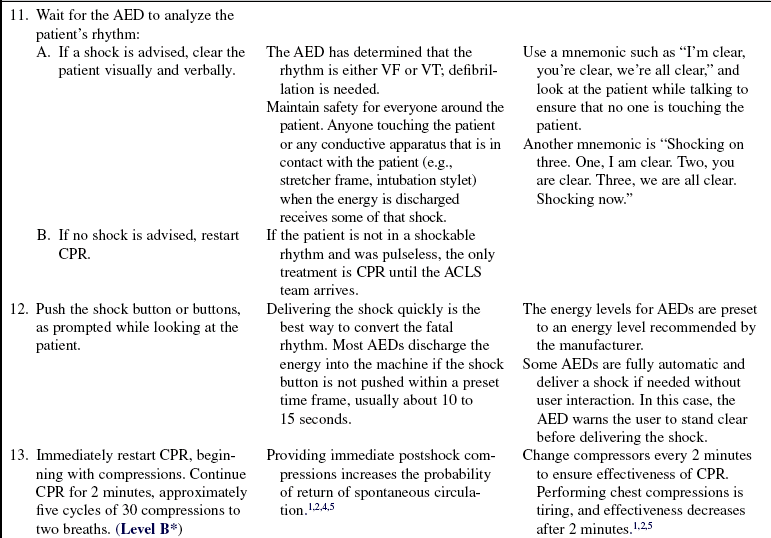
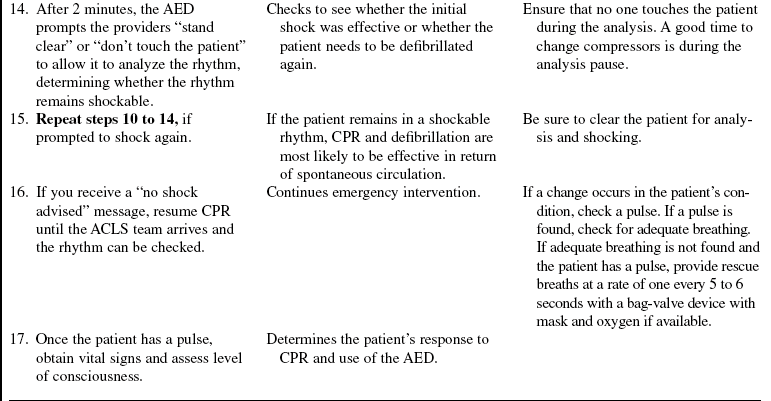
• Although defibrillation is the definitive treatment for VF and pulseless VT, the use of the AED is not a stand-alone skill; it is used in conjunction with CPR. CPR should be started as soon as the patient is found to be pulseless and not stopped until the AED has been turned on, the pads have been attached, and the machine is prompting the provider to “stand clear” or “don’t touch the patient.”1,2,5 Immediate postshock CPR starting with compressions has been documented to lead to increased return of spontaneous circulation and increased cerebral survival,4,5 which is why time is not taken to check for a rhythm or pulse after defibrillation.
• Ventricular fibrillation depletes the cardiac energy stores of adenosine triphosphate (ATP) more rapidly than a normal rhythm. The longer a heart goes without circulation, the more depleted its energy stores. In a heart with depleted energy stores, defibrillation is more likely to result in asystole because no fuel remains to support spontaneous depolarization or myocardial contraction. Effective CPR can supply the needed oxygen and energy substrates to the heart cells and allow them to return to a perfusing rhythm.4,5
• Three stages of VF are seen in cardiac arrest. The first phase is the electrical phase. During this phase, which is considered the first 4 to 5 minutes of VF, defibrillation is most likely to be effective, and the sooner the shock can be delivered the more likely it is to work. During the next 5 to 10 minutes after VF occurs, the hemodynamic or circulatory phase, a brief period of CPR may “prime the pump” and provide oxygen and energy substrate to the myocardial cells, improving the effectiveness of the defibrillation. If the patient is found during this phase, or if CPR is not ongoing when the defibrillator arrives, effective CPR needs to be administered for approximately 2 minutes, or five cycles of 30 compressions to two ventilations, before the shock. The metabolic phase starts 10 minutes after VF. During this phase, the cardiac cells have experienced global ischemia and energy depletion if no CPR has been initiated. CPR before defibrillation is more likely to be successful and needs to be used in conjunction with advanced cardiac life support (ACLS) therapies.4,5
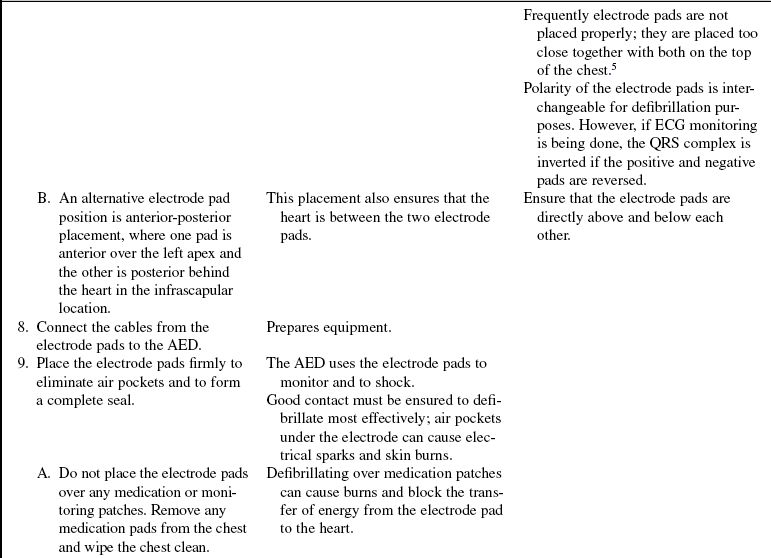
• The AED is attached to the patient with adhesive electrode pads. Through these pads, the rhythm is analyzed and a shock delivered, if indicated. If the AED recognizes VF or VT, visual and verbal prompts guide the operator to deliver a shock to the patient. The AED, not the operator, makes the decision about whether the rhythm is appropriate for defibrillation.
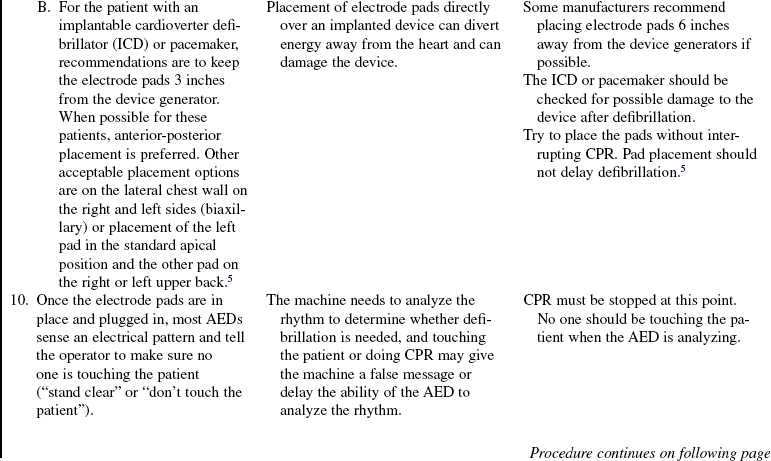
• The chance of the AED shocking inappropriately is minimal.1,5,7 The AED should be applied only to unresponsive, nonbreathing, pulseless patients. To keep artifact interference to a minimum, the patient should not be touched or moved during the analysis time.
• The mnemonic “PAAD” makes it easy for the rescuer to remember the steps of operation of the AED: “P” for Power on, “A” for Attach the pads, “A” for clear to Analyze, and “D” for clear to Defibrillate.
• Although AEDs are simple to use, healthcare personnel should be familiar with and technically competent in use of their AED.
• The AED is recommended for use in children ages 1 through 8 years if the child shows no signs of circulation. Approximately 5% to 15% of children in arrest have initial VF.1,5,6 Primary VF in children rapidly changes to asystole; rhythm detection and rapid defibrillation in children is most effective. It is best if the defibrillator has a pediatric switch or pediatric pads, which have an attenuator in the cord that decreases the amount of energy delivered. If pediatric pads are not available, adult pads should be used.1–3,5,7 With use of adult pads, ensure that they do not touch each other because this may cause electrical arcing and skin burns and divert defibrillation energy. The pads should be at least 1 inch apart. If the pads cannot be fit on the child’s chest in a lead two position, an anterior-posterior pad placement should be used.1–3,5,7,9 Never use pediatric pads on an adult or large child because the reduced energy levels delivered by these electrodes may not be effective for treatment of VF.
• The use of AEDs in prehospital settings has increased the success of defibrillation. The goal in the hospital should be to have the ability to defibrillate any person in cardiac arrest within 3 minutes or less of discovery. Placement of AED units in nonmonitored patient units and in public use areas of a hospital increases patient chances of survival.2,5,6,8,10,11 AEDs are also recommended to be placed in freestanding or ambulatory care settings.
• Many manual defibrillators that can be purchased have analysis capability that allows a tiered response (i.e., individuals with different skill levels can use the same defibrillator).
• Most AEDs in use in emergency response systems (EMS) or in the hospital have a method of recording the event, in the form of rhythm strip printouts, audio and event recording devices, data cards, or computer chips that can print an event summary.
• AEDs can be purchased with and without monitor screens. AEDs with screens may allow the provider with rhythm recognition skills to override the AED’s analysis and recommendations.
• An important safety issue an AED operator must address is the possibility of inadvertently shocking a bystander or other provider at the scene. The operator must clear the patient verbally and visibly, by looking at the patient from head to toe, before and during the discharge of the energy to the patient.
• All defibrillation programs need to include training for the potential operators. Training should include psychomotor skills, troubleshooting, equipment maintenance, and how to interface with ACLS providers. Providers have the responsibility to be familiar with the machine they will use.
• When a resuscitation team (e.g., 911 responders, code team, ACLS providers) arrives, the team assumes responsibility for monitoring and treating the patient.
EQUIPMENT
• Barrier device or airway management equipment (bag-valve device with mask and oxygen)
• At least two sets of adult defibrillation pads and potentially one set of child defibrillation pads
Additional equipment to have available as needed includes the following:
PATIENT AND FAMILY EDUCATION
• AEDs are used in emergency situations with limited or no time to educate the family about the equipment or the procedure. If family is present in the room during the arrest, a staff member should be assigned to keep the family informed of the procedures taking place and to offer support.  Rationale: Information provides education and support.
Rationale: Information provides education and support.
• Occasionally, after a sudden cardiac event, a patient may be discharged from an institution with an AED. In these situations, patient and family education is essential and should include information regarding performing CPR and technical competence with the AED.  Rationale: Education prepares the family for potential future emergencies.
Rationale: Education prepares the family for potential future emergencies.
 Rationale: AEDs are indicated for the treatment of patients in cardiac arrest.
Rationale: AEDs are indicated for the treatment of patients in cardiac arrest. Rationale: This action prepares the patient for placement of the AED electrodes and minimizes the risk of electrical burns.
Rationale: This action prepares the patient for placement of the AED electrodes and minimizes the risk of electrical burns.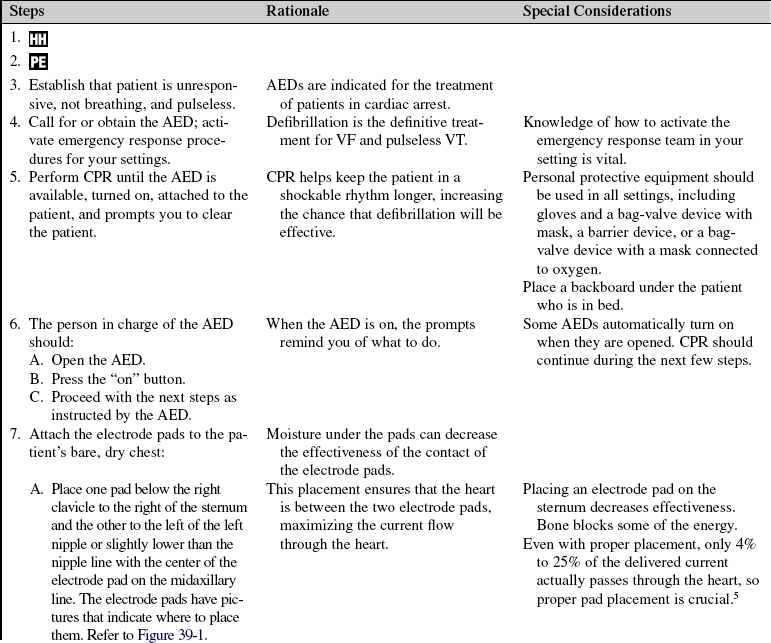
References
![]() 1. American Heart Association, Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care, part 4. adult basic life support. Circulation. 2005; 112(Suppl IV):35–46. [IV].
1. American Heart Association, Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care, part 4. adult basic life support. Circulation. 2005; 112(Suppl IV):35–46. [IV].
2. American Heart Association. Health care provider basic life support provider manual. Dallas: American Heart Association; 2006.
![]() 3. Atkinson, E, et al. Specificity and sensitivity of automated external defibrillator rhythm analysis in infant and children. Ann Emerg Med. 2003; 42:185–196.
3. Atkinson, E, et al. Specificity and sensitivity of automated external defibrillator rhythm analysis in infant and children. Ann Emerg Med. 2003; 42:185–196.
4. Berg, RA. Immediate post-shock chest compressions improve outcome from prolonged ventricular fibrillation. 0. Resuscitation. 2008; 78:71–76.
5. Field JM, ed.. ACLS resource text. for instructors and experienced providers. American Heart -Association: Dallas, 2008.
6. Gombotz, H, Weh, B, Mitterndorfer, W, et al, In-hospital cardiac resuscitation outside the ICU by nursing staff equipped with automated external defibrillators. the first 500 cases. Resuscitation 2006; 70:416–422.
7. Markenson, D, Pyles, L, Neish, S, and the Committee on Pediatric Emergency Medicine and Section on Cardiology and Cardiac Surgery. Ventricular fibrillation and the use of automated external defibrillators on children. Pediatrics 2007; 120:1368–1379.
![]() 8. Martinez-Rubio A, et al, Advances for treating in-hospital cardiac arrest. safety and effectiveness of a new automatic external cardioverter-defibrillator. J Am Coll Cardiol. 2003; 41(4):627–632.
8. Martinez-Rubio A, et al, Advances for treating in-hospital cardiac arrest. safety and effectiveness of a new automatic external cardioverter-defibrillator. J Am Coll Cardiol. 2003; 41(4):627–632.
![]() 9. Samson, R, Berg, R, Bingham, R, and PALS Task Force. Use of automated external defibrillators for children: an update; an advisory statement from the Pediatric Advanced Life Support Task Force, International Liaison Committee on Resuscitation. Resuscitation 2003; 57:237–243.
9. Samson, R, Berg, R, Bingham, R, and PALS Task Force. Use of automated external defibrillators for children: an update; an advisory statement from the Pediatric Advanced Life Support Task Force, International Liaison Committee on Resuscitation. Resuscitation 2003; 57:237–243.
10. Sandroni, C, Nolan, J, Cavallaro, F, et al, In-hospital cardiac arrest. incidence, prognosis and possible measures to improve survival. Intensive Care Med 2007; 33:237–245.
![]() 11. Zafari, M, et al. A program encouraging early defibrillation results in improved in-hospital resuscitation efficacy. J Am Coll Cardiol. 2004; 44(4):846–852.
11. Zafari, M, et al. A program encouraging early defibrillation results in improved in-hospital resuscitation efficacy. J Am Coll Cardiol. 2004; 44(4):846–852.
